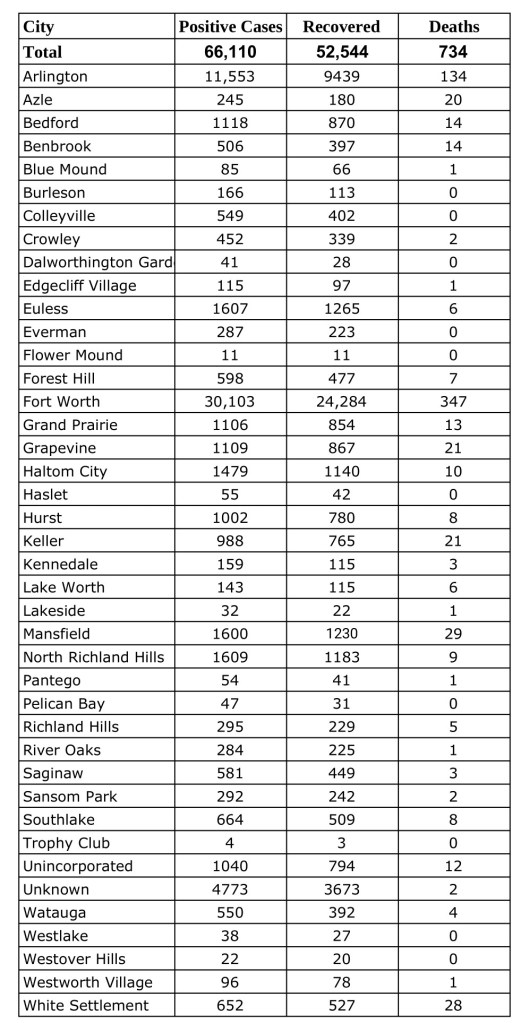
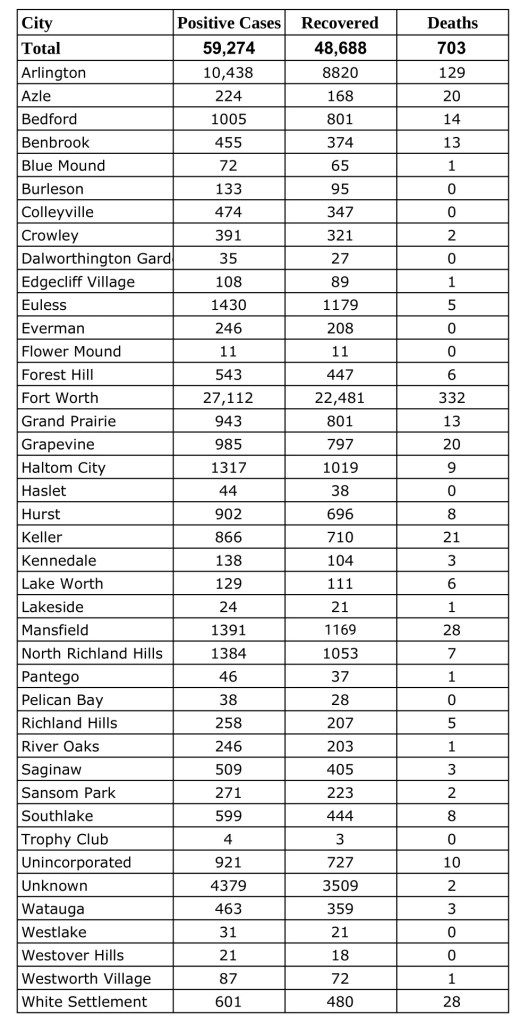
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Thursday, October 29, 2020.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
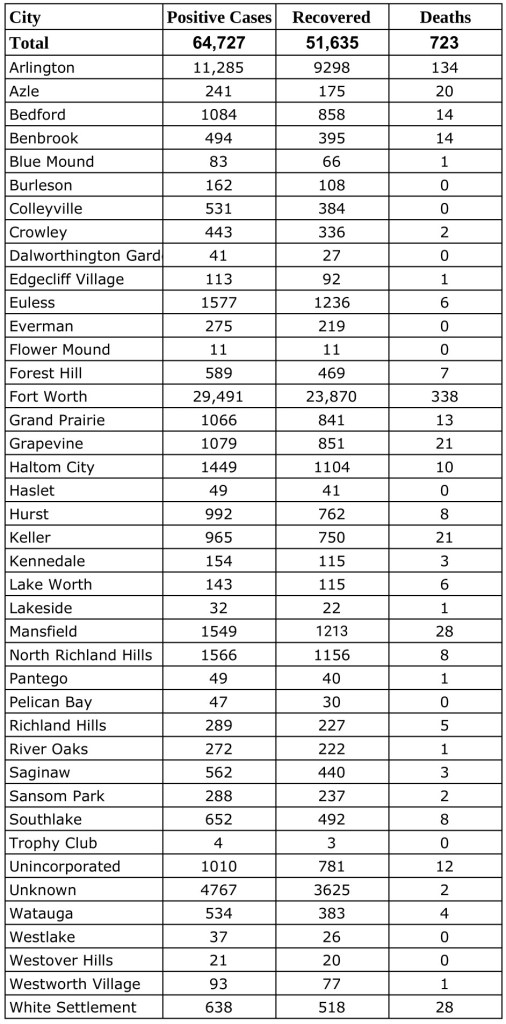
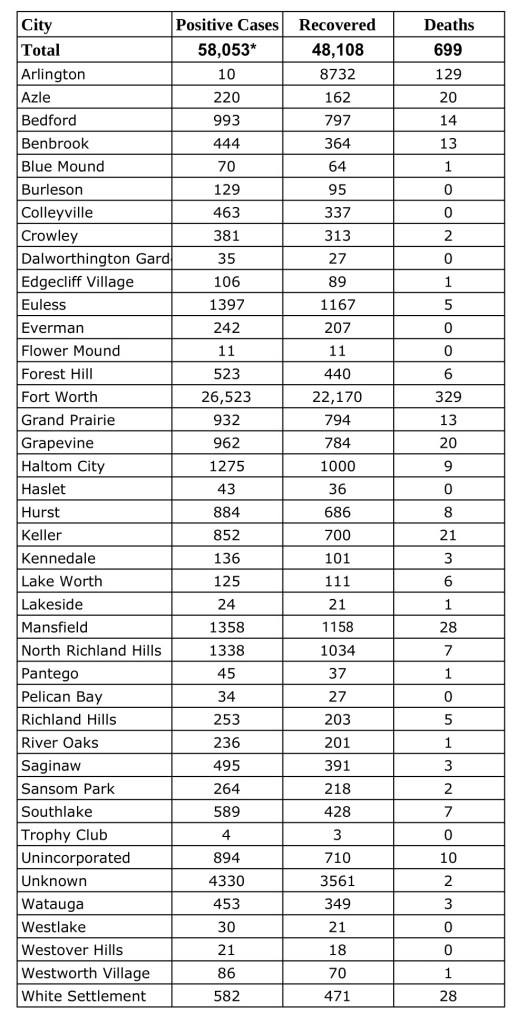
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Tuesday, October 27, 2020.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
This piece was originally published in the September/October issue of the Tarrant County Physician. You can read find the full magazine here.
by Tilden Childs, MD – TCMS President
When I was perusing the Wall Street Journal the other day, I ran across an article by one of my favorite writers, Daniel Henninger. He started his article with the following observation, “On Tuesday the New York City sky was clear, blue and filled with sunshine. That’s it for this week’s good news.” His article was not about COVID-19, but it prompted me to think that yes, there is some good news on COVID-19.
As I suspected early on, the COVID-19 pandemic is not going to be a short-term phenomenon with a “V” shaped medical recovery for the country, unlike the stock market (well at least some stocks). However, some recent developments do appear to be positive and hope for some return to normalcy has not been extinguished. The re-opening of the U.S. economy has been progressing, which is good, but unfortunately the infection rates have also increased. Parts of Texas, particularly in the Valley, are suffering. However, the mantra of “wear a mask or face covering, wash your hands frequently, and maintain physical distancing” seems to be working when rigorously applied. Even President Trump is taking the situation more seriously and now supports the wearing of a mask or facial covering.
The mortality rate from COVID-19 may be lower than was initially thought, but this is a complicated issue. As explained in an article in Nature: “Researchers use a metric called infection fatality rate (IFR) to calculate how deadly a new disease is. It is the proportion of infected people who will die as a result, including those who don’t get tested or show symptoms.” “The IFR is one of the important numbers alongside the herd immunity threshold and has implications for the scale of an epidemic and how seriously we should take a new disease,” says Robert Verity, an epidemiologist at Imperial College London. “Calculating an accurate IFR is challenging in the midst of any outbreak because it relies on knowing the total number of people infected—not just those who are confirmed through testing. But the fatality rate is especially difficult to pin down for COVID-19, the disease caused by the SARS-CoV-2 virus,” says Timothy Russell, a mathematical epidemiologist at the London School of Hygiene and Tropical Medicine. “That’s partly because there are many people with mild or no symptoms, whose infection has gone undetected, and also because the time between infection and death can be as long as two months.”1
Some potential reasons for the apparent recent decrease in the mortality rate were discussed in an article in The Atlantic: “COVID-19 Cases Are Rising, So Why Are Deaths Flatlining?”2
Deaths lag cases—and that might explain almost everything.
Expanded testing finds more cases, milder cases, and earlier cases.
The typical COVID-19 patient is getting younger.
Hospitalized patients are dying less frequently, even without a home-run treatment.
Summer might be helping—but only a little bit.
Let’s hope that #1 above is not correct! I would like to believe that the evolution of our understanding of the virus and the disease it causes, including a better appreciation for its variable severity and multi-organ involvement, has and will continue to result in more and better treatment options which are at least in part improving mortality and morbidity outcomes.
“This is really good news as it now appears that herd immunity may be the key to successfully mitigating the current crisis and controlling the SARS CoV-2 virus.”
Progress on developing a vaccine(s) is moving forward at an accelerated pace. This is the result of the National Institutes of Health and the Foundation for the NIH (FNIH) forming the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) partnership with the goal of developing “a collaborative framework for prioritizing vaccine and drug candidates, streamlining clinical trials, coordinating regulatory processes and/or leveraging assets among all partners to rapidly respond to the COVID-19 and future pandemics.”3 This represents an unprecedented cooperative alliance between government agencies and private industry to expedite the development of vaccine(s) as well as begin production of potentially successful vaccines in advance of final approval of the vaccine(s). At the time of writing this article, Phase III trials are about to begin for at least one of the vaccines under development. Availability of a vaccine(s) may be as early as late 2020 or early 2021.
This is really good news as it now appears that herd immunity may be the key to successfully mitigating the current crisis and controlling the SARS CoV-2 virus. Recent evidence suggests that immunity following infection is time limited and that significant long-term morbidity is believed to occur after recovery from the acute COVID-19 infection phase. This means that herd immunity generated by vaccinations rather than by community infections looks to be the key to getting the crisis under control and reducing the mortality rate and the long-term sequelae of community acquired infections.
I hope this Good News gives you reason to Keep up the fight and Keep the faith.
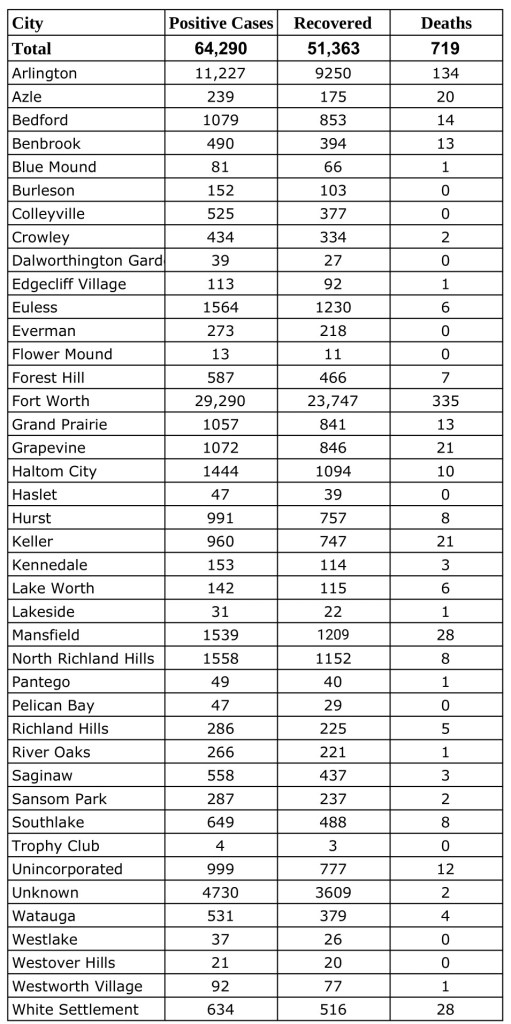
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Monday, October 26, 2020.Find more COVID-19 information from TCPH here.
These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
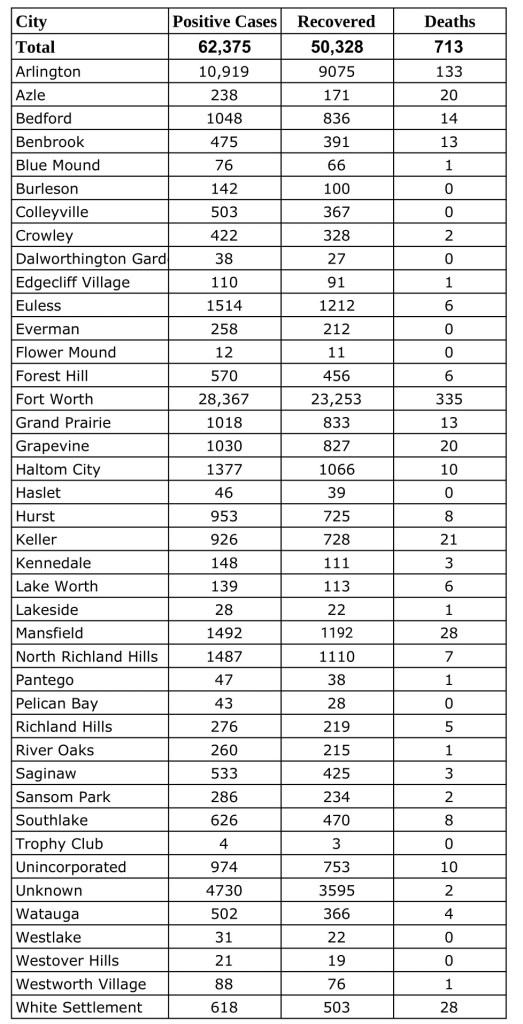
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Friday, October 23, 2020.Find more COVID-19 information from TCPH here.
These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
This piece was originally published in the September/October issue of the Tarrant County Physician. You can read find the full magazine here.
It happened twice in the same morning.
I saw two women for checkups that morning—their stories were so similar. Both older but not elderly, living alone, physically impaired needing a walker or motorized scooter, and always very crabby at their appointments. A litany of chronic non-specific complaints—fatigue, aching, headachey, etc. Honestly, I was not looking forward to their visits. They never seemed satisfied, and I never felt like I had helped them much. When I saw them both on the schedule that morning, I confess that I grimaced a bit.
But their telemedicine visits were just the opposite of their usual in-person visits. They both were happy, smiling, and relaxed. The conversations were easy and their questions were few. I anticipated much COVID-19 anxiety but found little; they were used to staying at home and hadn’t had to change their way of life much. They both just needed refills—I would have liked to have done a physical exam, but I really didn’t need to.
At the end of the morning, I wondered to myself what was different, and then it hit me. They didn’t have to physically come to see me, which so many of us take for granted but for them was likely a physically draining, frustrating, expensive, humiliating, and even painful experience. Wow. Was I humbled.
Telemedicine is a gift to some of our patients, such as parents stuck without childcare who have to bring multiple children along with them, people who lack reliable transportation, or elderly people who don’t like driving anymore but are embarrassed to ask for a ride. It can help someone two hours away who just needs a refill or a patient who can’t afford to miss work. I could go on and on; I’ve seen cases like every example I’ve given and I’m sure many of you have, too.
The coronavirus pandemic has added a new layer of urgency to the implementation of telemedicine. Physical distancing and shutdowns have made it extremely difficult, if not impossible, to see our patients safely face to face (especially when PPE is still hard to find). Telemedicine enables routine care to continue without the risk of exposure to the virus. It keeps medical offices safe and in business.
The AMA, along with many other organizations, has been developing telemedicine policy and recommendations for years. The AMA House of Delegates approved a report from the Council on Medical Services laying out principles for coverage and payment in June 2014.
An AMA survey in 2016 showed that 15 percent of physicians worked in a practice that utilized telemedicine in some way.1 But a far smaller percentage of actual patient encounters were done via telemedicine.
When COVID-19 struck and communities were shutting down all over the country, the telemedicine guidelines, reimbursement policies, and the work we had already done with CMS helped the organization be ready with their new guidelines for coverage and payment, which were initially released on March 17, 2020.
AMA had been working with the Physicians Foundation, the Texas Medical Association, the Florida Medical Association, and the Massachusetts Medical Society to create the Telehealth Initiative to provide a wide array of assistance for physicians to implement telemedicine in their practices.2 The launch of the program was not scheduled until later in the year but instead was moved up to March 19, 2020, just two days after the CMS announcement.
Virtually every medical society in the country now has guidance available for physicians on using telemedicine.
However, the current telemedicine coverage and payment program will only stay in effect as long as there is a national emergency, which has now been extended to the end of October 2020. Of course, we all know that COVID-19 will not be gone then, so AMA is working with state and specialty societies to lobby Congress for permanent solutions.
I believe that every specialty will develop its own guidelines for the appropriate use of telemedicine going forward, and every practice will utilize telemedicine to some degree.
The genie is out of the bottle. Let’s hope it stays that way. We deserve to be compensated fairly for services regardless of location, and our patients deserve the ease of access.
The following deadlines and extensions are in effect during the COVID-19 pandemic.
Through Oct. 23
Several Medicaid and Children’s Health Insurance Program(CHIP) flexibilities, including paying for Texas Health Steps (THSteps) medical checkups via telemedicine and CHIP copay waivers expired.
Through Oct. 31
Cigna is extending certain cost-share waivers for COVID-19 screening, testing, and treatment, including telehealth screening.
Through Dec. 31
Texas-regulated insurers must continue to pay for telemedicine services, including mental health visits, at the same rate as in-person visits. The extension was part of an emergency rule that was set to expire Sept. 12.
Aetna is extending coverage for commercial telemedicine service, including audio-only visits. Cost share waivers expired Aug. 4.
Blue Cross Blue Shield of Texas is extending certain cost-sharing and telemedicine waivers for state-regulated, fully insured HMO and PPO members and Medicare members.
To help you understand all of the changes to telemedicine during the pandemic, the Texas Medical Association has published up-to-date information for each type of payer.
Stay up to date with the latest news, resources, and government guidance on the coronavirus outbreak by visiting TMA’s COVID-19 Resource Center regularly.
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Sunday, October 18, 2020.Find more COVID-19 information from TCPH here.
These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Friday, October 16, 2020.Find more COVID-19 information from TCPH here.
These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
This piece was originally published in the September/October issue of the Tarrant County Physician. You can read find the full magazine here.
I was 13 years old the last time that I experienced a summer break, because it was that summer that I decided that I wanted to be a physician. I spent every summer after that through high school at the Volunteer Department of the nearest Level I Trauma Center in East Texas. If I wasn’t volunteering I was shadowing, and if I wasn’t shadowing I was scribing or taking classes that would prepare me for medical school. It became a constant cycle, month in and month out for 11 years. Every one of my spring breaks, winter breaks, and summer breaks was jam-packed with exciting new medical adventures, classes, or some other activity that was someday going to get me into medical school and ultimately help me become a physician. As crazy as it sounds, my story is not unique. This is the path for many students, former, current, and future, who pursue a career as physicians. This is a way of life that we gladly accept, because for many of us the idea of doing anything else is much more depressing than spending every break of our youth working towards our future career.
I was all geared up to spend the summer after my first year of medical school the same way. I had two in-hospital research projects lined up, was interviewing for a pediatric research program to review case studies and publish reports on the cases, and I was already looking for a summer job to bring in a little extra income during what I considered my “slow” month between the two academic years. Then, in an instant, a global pandemic hit, all my plans fell apart, and I was left with a very empty calendar during a period that was supposed to be a time for me to check all of the boxes that residency programs would want to see completed by the time I apply just three short years from now. When the initial shock wore off that a virus was capable of shutting down medical programs created and run by very people who live to combat these same types of diseases every day, it was like I had stepped into the sunshine for the first time in 11 years. As I began to read about the attempts of countries all over the world to contain and combat the virus, I was struck by an unexpected common theme in the rest of the world that I felt within myself: rejuvenation.
There were stories about nature being able to cleanse itself once people were no longer allowed to pour waste into it every day. Families were spending more time with one another at home, and smiles were being shared through technology all across the world because people were no longer able to go, go, go. Self-care began to emerge at the forefront of peoples’ minds, and I began to understand what it meant to take a step back and soak in the moments. I started cooking dinner every night, I read books on history and got outside every day. At a time when uncertainty was the norm and we were all scared, I spoke with colleagues and friends who were learning and growing personally outside the realm of medicine into better spouses, friends, and students. With this fresh new start that we received, we have been able to go back to school refreshed and ready to learn about medicine and people instead of being burned out and emotionally exhausted. During the time that our medical lives stood still, our mental and emotional health was able to re-blossom into excitement about life, medicine, and being the physicians that we are destined to become.