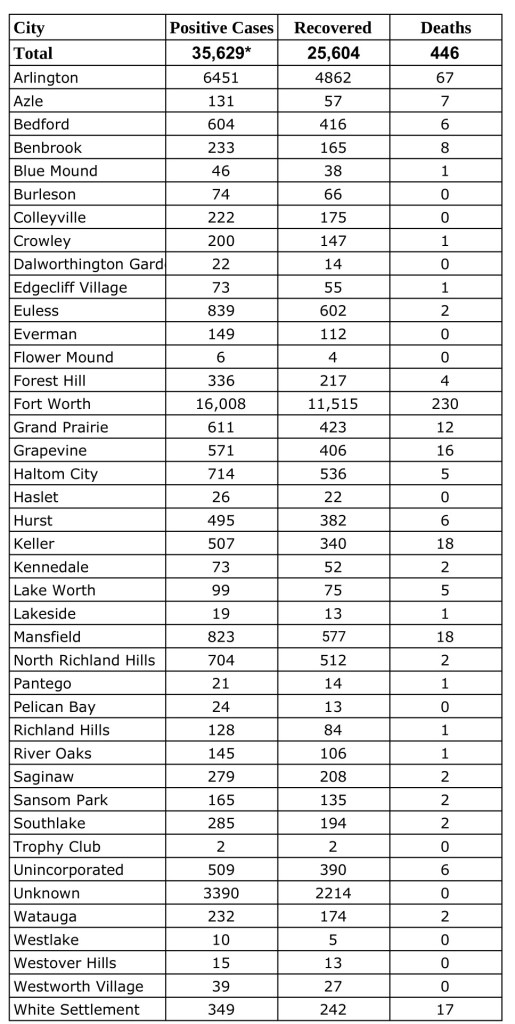
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Friday, August 14, 2020.Find more COVID-19 information from TCPH here.
* These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
With the return of August heat and daily temperatures now approaching 100 degrees, Tarrant County Public Health reminds residents to avoid heat-related illness.
“The risk of heat injury or death is at its worst when high temperatures continue over multiple days,” said Public Health Director Vinny Taneja. “People suffer heat-related illness when their bodies can’t compensate and properly cool themselves. Natural cooling occurs when people sweat, but under some conditions, sweating is not enough, and a person’s body temperature rises rapidly.
“While the elderly, young children and people dealing with chronic ailments are usually the first to suffer from the heat, I urge everyone to take precautions,” Taneja said.
Among those precautions:
Never leave children or animals in parked vehicles. When outdoor temperatures are high, children and animals left inside parked cars can be overcome by heat within minutes.
Minimize exposure. Being outside in high temperatures for prolonged periods puts anyone at risk of heat injury, especially if active in outdoor athletic programs, youth organizations or schools.
Avoid dehydration. Water is the most critical beverage a person can drink to prevent heat injury. Develop the habit of drinking water every hour when it’s hot outside — even if you are not thirsty. Avoid drinking alcohol on hot days.
Maintain adequate ventilation/air conditioning. Some people turn off their air conditioning, do not run it long enough or may not have access to fans or other devices that circulate cool air. Unless people have a high tolerance for heat, this practice puts them at risk for heat injury.
The elderly are most at risk. Neighbors, friends and family should regularly check on the elderly when temperatures are high for multiple days.
Before the COVID-19 pandemic began, medical professionals, including surgeons, had already been utilizing social media for networking purposes. An example is the monthly Association of Women Surgeons Tweet Chat (@womensurgeons). Students can participate, and I personally have been able to meet resident and attending physicians at various residency programs through these chats. This interaction provides me and other applicants the opportunity to network before interview season begins. Without audition rotations, these interactions will become highly valuable. Having the ability to connect with program directors, residents, and attendings through these chats may be the difference in being offered an interview or not.
Fourth-year students are also concerned the virtual interview process will not provide us an accurate representation of residency programs. One emergency medicine (EM) resident physician echoed this concern and tweeted asking EM programs to share information about their program, including name, a unique aspect of that program, and information about the program’s city. Numerous residents have replied to his tweet, allowing rising fourth-year medical students to gain insight about EM programs from all around the country. Seeing the success of this tweet, I decided to ask for general surgery residents to share more about their programs. The responses have allowed me and other aspiring surgeons to learn about more than 25 different general surgery programs across the country.
Twitter is not only a means for residencies to share information about their program; it is also a way for them to learn about applicants. The biography section is an opportunity for us to provide more personal information, including our medical school, hobbies, and interests. I have been expressing myself through Twitter by re-tweeting surgery research, posting about cooking and baking, and sharing funny videos to show my sense of humor. Programs want to know more about applicants than our board scores, and thoughtful biographies and tweet content can show a residency program more about a student and what we can bring to a program.
For this year’s rising fourth-year medical students, it is more important than ever to be active on social media. This engagement is enabling us to network, learn about residency programs, and show programs who we are. With the help of Twitter and other technologies, residencies and medical students alike will be able to interact and form relations in spite of physical distance.
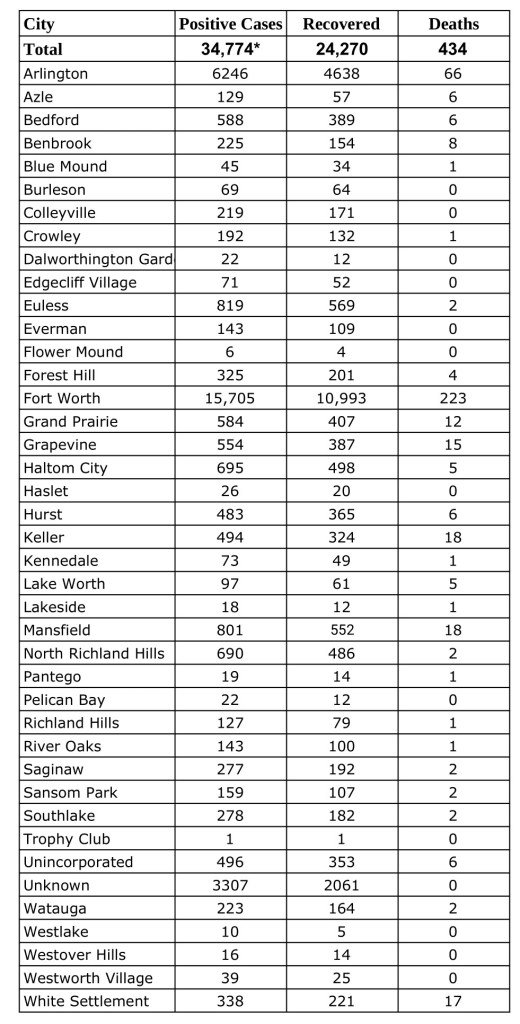
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Wednesday, August 12, 2020.Find more COVID-19 information from TCPH here.
* These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
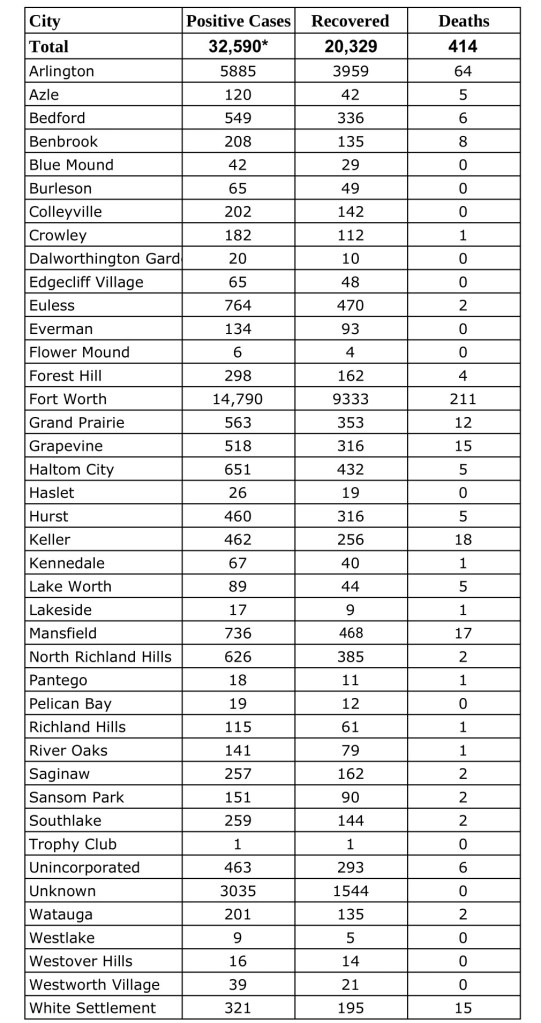
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Tuesday, August 11, 2020.Find more COVID-19 information from TCPH here.
* These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
Governor Greg Abbott and the Texas Health and Human Services Commission (HHSC) announced that the federal government has further extended the deadline to apply for the CARES Act Provider Relief Fund.
The deadline has now been extended to August 28, 2020 for Medicaid and CHIP providers as the state responds to the COVID-19 pandemic. In addition, starting August 10, 2020, Medicare providers can apply for additional funding from the $20 billion portion of the $50 billion Phase 1 Medicare General Distribution.
The City of Fort Worth and Tarrant County are expanding COVID-19 testing for residents throughout the city.
Tests will be available at these locations:
Tuesday, Aug. 11, FWISD Scarborough-Handley Field parking lot 6201 Craig St.
Wednesday, Aug.12, Tarrant County College-Northwest Campus, 4801 Marine Creek Parkway.
Thursday, Aug. 13, Beth Eden Missionary Baptist Church, 3208 Wilbarger St.
Friday, Aug. 14, Christ Church Fort Worth Assembly of God, 5301 Altamesa Blvd.
Tests will be available at these locations for one day only before the test site moves to a new location.
Tests will be available from 8-11 a.m. and 2-5 p.m. daily. Tests at all sites are available by online appointment. Residents who do not have access to a computer may call 817-248-6299 to schedule an appointment.
“Fort Worth will continue to collaborate with partners to ensure COVID-19 testing is readily available and accessible to all residents throughout all of Fort Worth,” said Mayor Betsy Price. “Testing plays a critical role in our continued efforts to prioritize public health, keep Fort Worth’s economy open and get our children back in school.”
In coming weeks, additional sites will be added as suitable locations are identified.
“It is vitally important that we bring more testing to Tarrant County,” said Tarrant County Judge Glen Whitley. “We’re excited to expand our partnership with the City of Fort Worth to add more testing across the county, making it easier for residents to get tested.”
The city’s emergency response volunteers will continue to staff two COVID-19 testing sites, which are currently open:
J.P. Elder Middle School, 709 N.W. 21st St. 8 a.m.-noon.
Dickies Arena’s Chevrolet Parking Garage, 3464 Trail Drive. 2-6:30 p.m.
City staff from Police, Fire and Code Compliance departments, along with certified city volunteers for emergency response, are staffing the sites and guiding patients through the self-administered saliva sample collection process. Tests are offered at no cost to the public; however, insurance information is collected, where possible.
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Friday, August 7, 2020.Find more COVID-19 information from TCPH here.
* These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
By now you’ve probably treated a lot of COVID-19 patients, many of whom have recovered from the illness.
Although employees are not required by law to present a letter from a physician clearing them to return to work, many employers request one.
If your practice doesn’t already have such a letter, the Texas Medical Association has created one that you can customize for your practice.
The letter, which is available here, outlines guidance from the Centers for Disease Control and Prevention (CDC) on when employees who have exhibited symptoms or who have tested positive should return to work. It also explains a negative swab test is not required by law for employees to return to work.
The letter is one of several COVID-19-related documents TMA has created that you can customize for your practice’s and patients’ individual needs. Those resources as well as up-to-date news, information, and tips can be found on the TMA COVID-19 Resource Center.
Dr. Susan Bailey, AMA President, presented this speech on June 7, 2020, when she was installed as the 2020-2021 president of the American Medical Association:
The inauguration of a new AMA president is typically a very formal, black-tie affair with great celebration and fanfare. In my case, my family and close friends were all excited and ready to fly to Chicago to celebrate with me.
I had a beautiful gown and Broadway entertainment and red velvet cake for dessert all picked out.
My grandson was going to look so adorable in his tux . . . just like his daddy and his uncle did at his age when I became president of the Tarrant County Medical Society.
I was planning one final bow with my predecessors, Drs. Patrice Harris and Barbara McAneny, capping our historic year with three consecutive women presidents.
But the coronavirus had other plans. And seemingly overnight, our world changed.
So here I stand, in a nearly empty studio, talking to you through a video screen.
And that’s okay. As physicians we understand better than anyone how a health emergency can disrupt even the most carefully thought out plans.
No matter the circumstance, I am grateful to address you for the first time as AMA president, and I am so honored to carry the mantle of leadership for this organization I have been proud to serve for 40 years.
On this journey to become AMA president, I’ve been asked who my heroes were growing up. We hear about heroes every day now, it seems.
But what IS a hero?
Who were my heroes?
I was never particularly into make-believe superheroes as a kid. It was real people in my life whom I most admired and emulated; the people who inspired me and pushed me to a life beyond anything I could have imagined for myself.
My heroes were my physicians.
They were my first heroes . . . and they’re still my heroes.
I had significant allergies and asthma as a little girl, and my allergists were a guiding light in our family. In fact, the McGovern Allergy Clinic in my hometown practically raised me, instilling in me a passion for medicine and teaching me the basics about working in a medical office—how to take a patient’s history, perform allergy testing . . . and how to give a damn good shot.
I grew up in the shadow of the Texas Medical Center in Houston, and many of my friends’ dads were physicians. At that time, in the 1960s, it was always the dads. Thankfully now, it’s moms too.
Although I rarely saw those physicians, I idolized them. After my father had double cardiac bypass surgery in the early ‘70s, one thing that sped his recovery was taking daily walks by the home of his surgeon, Dr. Jimmy Howell, in the hope that one day the doctor would see him and be proud of him.
One day he did see my dad, and he was indeed proud of him . . . and that kept daddy walking the rest of his life. Oh, how daddy—and our hero Dr. Howell—would be proud today.
What we’ve witnessed in this pandemic and what we know from history is that heroes are defined by their ability to adapt to a changing world, to follow a righteous cause, to overcome immense challenges, and to be changed by it forever.
The author Joseph Campbell discusses this in his book, Hero with a Thousand Faces, which describes the mythological hero’s journey in 12 stages, establishing the classic story line in everything from the original Star Wars trilogy and Harry Potter to The Wizard of Oz.
As Campbell describes it, a hero starts off in the ordinary, familiar world, but gets a call to adventure. Think of a humble farm boy on Tatooine getting the call from Obi Wan Kenobi to help save Princess Leia.
At first, our hero is reluctant, even fearful. But a supernatural force or mentor comes along and brings out the most in them. A threshold is crossed, and the adventure begins. Dorothy skips down the Yellow Brick Road.
On the way, our hero encounters challenges, finds allies, and makes enemies.
Eventually, our he or she arrives at the ultimate test. Harry Potter confronts Voldemort face to face. This is a dangerous place . . . a dark place . . . a place where survival is as important as the ultimate goal. There is a fight to the death.
Somehow, someway, the hero prevails, but the story is far from over. Going back to ordinary life is not easy, and there are many bumps in the road. But in the end, our hero emerges, transformed.
Luke is a Jedi Master. Dorothy returns to Kansas. Harry lives out his life as a benevolent wizard.
That’s the hero’s journey . . . and it’s been told a million times in a million different ways.
A hero’s journey is our journey . . . a physician’s journey.
You start off as a young student, maybe already in another career, but at some point you hear the call of medical school.
Somebody gives you a hand, maybe a teacher or a co-worker, and miraculously you’ve arrived as a first-year medical student. You feel like an imposter at first, and you wonder if you have made the biggest mistake of your life.
Through wit and resourcefulness, you figure out how to be successful. You don the white coat and you make lifelong friends, all the while confronting clinical challenges that you fear might break you.
At some point you confront the ultimate test. Maybe it’s having a relationship suffer because your priorities have changed. Maybe it’s not matching into the specialty or program you thought you wanted. Maybe it’s losing your first patient.
You’re in a dark place and it seems there is no way out. But you keep going.
You find your way out of the darkness and you emerge a better physician and a stronger person for having endured these trials. You realize that you are making a difference in people’s lives. You are saving lives.
You’re not the same person you were before you went to medical school. You are a physician . . . and you’re following the hero’s journey.
But here’s the thing – even heroes need allies on their sides. Luke needed R2D2. Harry Potter needed Hermione and Ron. Dorothy needed her ragtag crew.
There isn’t a single person I know who walks this journey alone.
My own allies are far too many to mention and thank in my limited time, but they include my husband Doug, who has been my greatest supporter and partner on this journey. They include my sons Michael and Stephen Wynn and Michael’s partner, Hannah Guel, my precious grandson Jackson, my sister Sally Rudd Ross, and her beautiful family.
They include my wonderful partners, Drs. Robert Rogers and Drew Beaty, my medical assistant Joyce Hayes, and all of their families, and my lifelong friends from Texas A&M University and the Disciples of Christ church.
And it of course includes my family in organized medicine; the Tarrant County Medical Society where I got my start, the Texas Medical Association, and my allergy and pediatric specialty societies the ACAAI, QuadAI, and the AAP. Special thanks to Dr. Melissa Garretson for your friendship, hard work, and dedication to help me make this journey possible.
It also includes my family at the AMA, and all of those colleagues, confidants and executives along the way who have mentored me and become dear friends. I have not named you all by name, but please know you are forever in my heart.
And like any hero’s journey, ours in medicine is simple:
Let doctors be doctors.
After more than 30 years in a small, private practice, I’m a passionate defender of the independent physician, and, like the AMA, I’m determined to remove all those obstacles that have come between us and our patients.
Insurer and government mandates. Decreasing payments and increasing demands. Burnout and physician suicide. And the coronavirus pandemic has made all of these problems more acute.
We need the power of the AMA on this journey.
I believe involvement in organized medicine is a professional obligation—taking good care of our patients requires much more from us than the time we spend with them in an exam room.
It requires advocacy at the highest levels to fight against the quagmire of regulation and for the support we need to sustain private practice during a pandemic that is threatening its very survival.
It requires us to confront insurance companies and all their familiar tricks that seem to raise insurance premiums year after year without spending a dime more on patient care.
At times I fear that our nation’s dysfunctional health system is held together only by the oath that we take when we graduate medical school . . . the pledge to always put the needs and interests of our patients first.
Whether you took the Hippocratic Oath or, as in my case, recited the Prayer of Maimonides, these words demonstrate our loyalty to public service, to the pursuit of science and knowledge.
These words bring purpose and meaning to our work, elevating it from a vocation to a profession.
We are on a new quest that none of us expected – living and working in a world that may be changed forever in an angry, divided nation that needs our leadership. But we need not fear the dark times on our journey.
We need only to lean on one another, to take care of each other, and to keep our eyes fixed on the horizon.
We will get through this pandemic.
We will continue to fight for our patients and for the practice of medicine.
This is our journey . . . and we will walk it together.