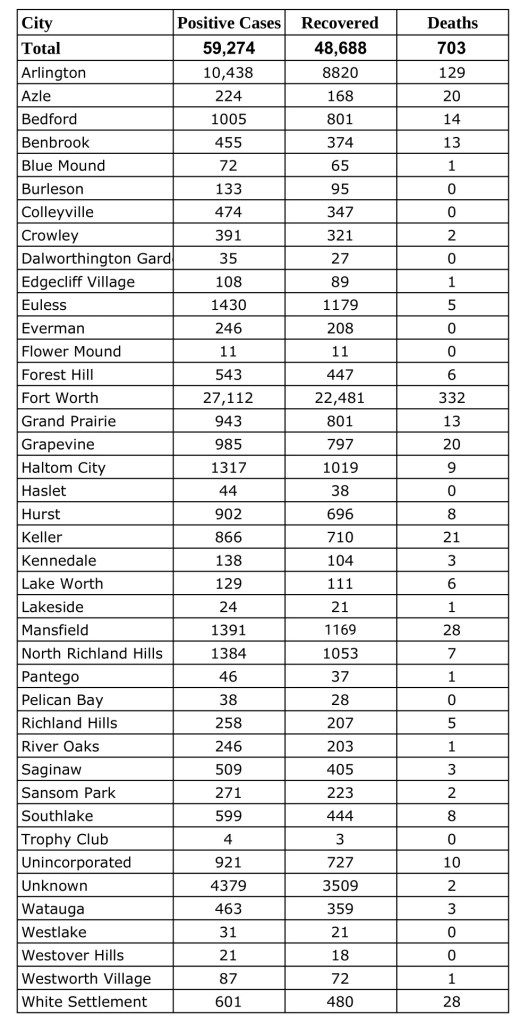
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Sunday, October 18, 2020.Find more COVID-19 information from TCPH here.
These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
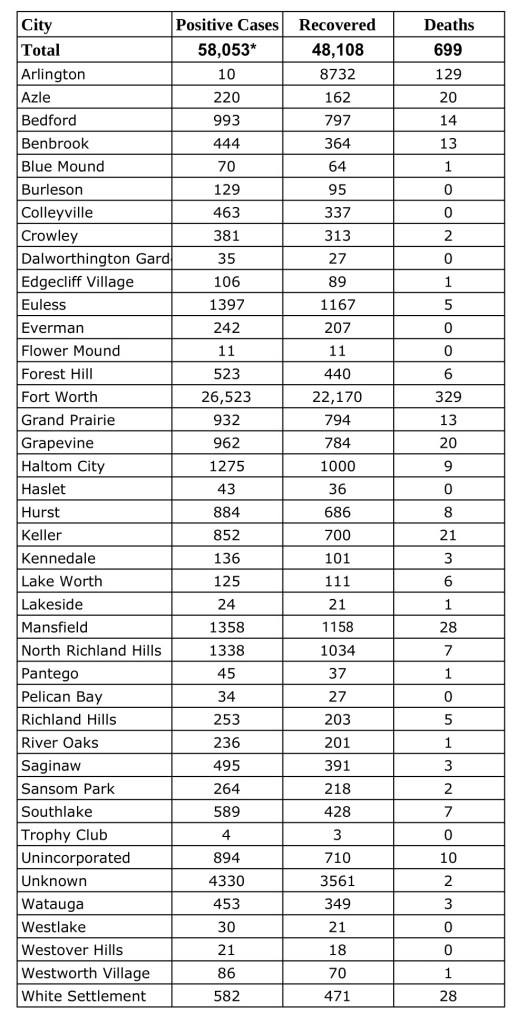
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Friday, October 16, 2020.Find more COVID-19 information from TCPH here.
These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
With fall festivities in full swing and Halloween fast approaching, physicians in North Texas have broken down traditional activities into low, moderate, and high-risk categories according to CDC guidelines.
“Some traditional Halloween festivities need to be modified this year to avoid high-risk activities involving close contact, but there are still plenty of fun holiday activities to enjoy with your kids,” said Dr. Beth Kassanoff, Vice Chair of the North Texas Medical Society Coalition and President-Elect of the Dallas County Medical Society. “Continue to stay physically distanced, wear a cloth or disposable surgical mask, and wash your hands, but have fun with the holiday.”
As with all activities during the COVID-19 pandemic, participants should wear a cloth face covering, maintain physical distance, and wash their hands frequently while participating in any of these activities. Additionally, wearing a cloth face covering along with a traditional costume mask over or under it should be avoided.
Low-Risk Activities:
Carving and decorating pumpkins with members of your immediate household or with friends at tables 6-10 feet apart, separated by household.
Halloween scavenger hunts with members of your immediate household.
Decorating your home.
A virtual Halloween costume contest with your school, friends, and/or family.
A physically distanced Halloween movie with an outside screen and projector, or a family movie night inside with the members of your immediate household.
A pinata at home with members of your immediate household.
Moderate-Risk Activities:
A small group (less than 10 people) outdoor costume parade while maintaining physical distance and wearing a cloth face covering.
Individual goody bags set up on an outside table for grab-and-go trick or treating. Consider leaving hand sanitizer for added safety.
Visiting pumpkin patches while maintaining physical distance and wearing a cloth face covering.
High-Risk Activities:
Traditional trick or treating door-to-door.
‘Trunk or Treat’ events and Fall Festivals and carnivals.
Haunted Houses.
Hayrides.
Outdoor gatherings that do not allow for physical distancing or any indoor parties or events with individuals outside your immediate household.
Some steps you can take to mitigate concerns might include:
Get your flu shot at least two weeks before Halloween.
Use hand sanitizer regularly and avoid touching your face.
Wear a cloth face covering if you are participating in any Halloween activities with people other than those living in your home.
Wash your hands well before eating.
Do not participate in activities with other people if you are sick or have been exposed to COVID-19.
About North Texas Medical Society Coalition:
The NTMSC represents more than 11,500 physicians in the communities of Collin-Fannin, Dallas, Denton, Grayson, and Tarrant County. Founded in 2020, the NTMSC works with community healthcare partners, including public health departments, hospitals, and business leaders, to advise on medical recommendations to serve the health care needs of the residents of North Texas.
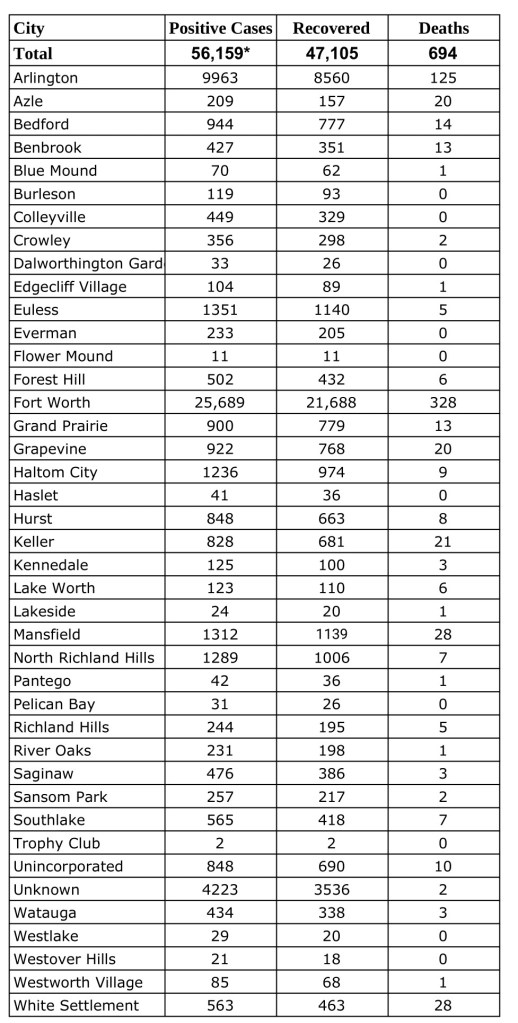
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Wednesday, October 14, 2020.Find more COVID-19 information from TCPH here.
These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
Early voting starts in Texas this week. Physicians urge all Texans to play it safe as they fulfill their civic duty, reminding everyone that it is possible to vote safely during a pandemic.
“Voting can be made safe by following the public health guidelines,” said Diana L. Fite, MD, president of the Texas Medical Association (TMA). “A little planning goes a long way.”
With the coronavirus still actively spreading in Texas, some elderly patients and Texans with disabilities wonder if it’s safe for them to vote in this year’s election, since they are most at risk for serious illness if they catch COVID-19.
Texans might have two options to vote: an individual might qualify to vote by mail, or he or she may vote in person.
“For those over 65 years old or who have chronic illnesses, it would be preferable to stay at home and send off an application for a mail-in ballot,” said Dr. Fite. “It’s certainly safer for these people to vote at home and mail their ballot than to venture out among crowds.” Any registered voter 65 years or older on Election Day or with a disability may vote early by mail in a Texas election.
The Texas Secretary of State has information and instructions about how to apply to vote by mail. Tip: The voter’s local voting clerk must receive an application for a mail-in ballot by Friday, Oct. 23.
For Texans opting to vote in person, there are options as well.
The early voting period runs Tuesday, Oct. 13 through Friday, Oct. 30. During this period, registered Texans can vote in person at any polling location in their home county. Voters might consider looking online for less-busy polling places and times, to avoid crowds.
Dr. Fite recommends early voting if possible to avoid any unforeseen problems. “If a person is sick on Election Day, that person should not go out to vote,” said Dr. Fite. “Instead, early voting is a consideration to avoid that possibility from occurring.”
On Election Day, Nov. 3, voters registered in a county that participates in the Countywide Polling Place Program may vote at any polling location in the county. If someone’s county does not participate in that program, he or she must vote in their own precinct on Election Day.
Whether voting early or on Election Day, physicians urge everyone to plan ahead and practice the same public health best practices as if they were going to the grocery store or anywhere else in public.
“Wash hands or use sanitizer before and after voting, try to stay 6 feet from others, and wear a mask,” said Dr. Fite. Simply maintaining space while waiting in line to vote can help prevent the spread of germs.
Physicians remind everyone of these tips for voting in person:
Stay at least six feet away from others;
Bring your own pen, pencil, or stylus;
Wash or disinfect your hands before and after voting;
Wear a face mask (you might have to remove it briefly for the election judge to confirm your identity); and
Stay home if you’re sick.
TMAis the largest state medical society in the nation, representing more than 53,000 physician and medical student members. It is located in Austin and has 110 component county medical societies around the state. TMA’s key objective since 1853 is to improve the health of all Texans.
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Tuesday, October 13, 2020.Find more COVID-19 information from TCPH here.
These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Monday, October 12, 2020.Find more COVID-19 information from TCPH here.
These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
This piece was originally published in the September/October issue of the Tarrant County Physician. You can read find the full magazine here.
As is tradition, despite what may be going on in the world (global pandemic, public demonstrations, etc.) every year, sometime in late June or early July, the wheel of medical education continues to turn. The TCU and UNTHSC School of Medicine continued this cycle on July 6, 2020. And just like that, our school went from one class to two, officially welcoming its second class of 60 medical students. The students in the Class of 2024 are from 18 states within the U.S., with 38 percent of them from Texas. Fifty-five percent are male and 45 percent are female. The new students come from 45 different undergraduate higher education institutions.
And just like that, there were two, and we continue our journey of developing a new medical school.
Similarly to our now second-year medical students, our first-year medical students are having to discover the brave new world of virtual medical education due to COVID-19. Despite this distance, our new students show the same enthusiasm for diving in that is always present in a brand-new class. This enthusiasm helps to invigorate those of us involved in medical education, and it helps us to continue to appreciate the honor it is to be a physician as well as an educator.
I was fortunate to participate in an interprofessional education event with our new first years as well as senior nursing students from TCU, held virtually of course. Our students were able to work through the concepts of communication in the clinical environment with the nursing students. They were also able to gain insight from the nursing students who have already been working in the clinical environment. It reminds me how important it is that our learners start working together while training. We highlight the concept that medicine is a team sport, and we must work together to obtain optimal outcomes for our patients.
The medical education wheel continues to turn.
By the time you read this, our second-year students will have completed the first of three phases of our curriculum, which is traditionally considered the basic science content. After years of planning and a global pandemic occurring more than halfway through our first year, it is hard to believe that this milestone has already occurred. Our students will now begin the transition to the clinical learning environment (barring any changes that may occur due to COVID-19). They will have the opportunity to step away from the computer screen and step back onto the campus for their Transition to the LIC course.
They will first get acquainted with the new normal of wearing a mask while trying to interact and gain rapport with simulated patients. They will also practice and hone clinical skills that were not able to be taught virtually. They will learn new procedures and have opportunities to practice. They will discover different medical environments, such as the operating room, labor and delivery, the inpatient setting, the emergency room, and outpatient clinic, and how they will play a role in those settings. They will also learn about the appropriate donning and doffing of personal protection equipment as well as telehealth that is now more commonplace due to the COVID-19 pandemic.
Once they complete their transitions course, the students will move into the hospital setting to continue their education. We are grateful to our physician and hospital partners in the community who have worked with us to bring our students into their clinical practice and hospital settings. To quote Sir William Osler, “To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.”1
And just like that, the medical education wheel continues to turn.
References 1. Boston Medical and Surgical Journal, January 17, 1901, page 60.
By Catherine Colquitt, MD, Tarrant County Public Health Medical Director
This piece was originally published in the September/October issue of the Tarrant County Physician. You can read find the full magazine here.
There is still much controversy regarding efficacy of masking during the COVID-19 pandemic, so I reviewed some of the thousands of peer-reviewed scientific articles addressing this topic since SARS exploded onto the world stage in 2003. Epidemiologists, infection perfectionists, and most if not all practicing physicians field questions from patients, friends, health care workers, and first responders about masking, and, while a comprehensive literature survey is beyond my scope, I came away from my reading heartened by evidence which clearly supports masks as a source control measure (a means of preventing transmission of infection from a source to others) AND endorses the use of masks, especially respirator and surgical masks, to PROTECT the wearer as well.
Masks, along with social (or physical) distancing, and hygiene (hand and surface disinfection, and cough and sneeze control) are the mainstays of control of droplet-spread pathogens and are critically important when COVID-19 hospital resources are strained, when treatments are reserved only for the sickest of those hospitalized, and in the absence of a vaccine or treatment for outpatients with COVID-19.
The science of evaluating masks is very complicated and typically involves at least three parameters: filtration efficacy (percentage of particles prevented from escaping the wearer’s mask), the pressure gradient across the mask (affects filtration efficacy and the comfort of the wearer), and fit, or face seal, of the mask on the wearer (droplets can escape more easily around looser edges of the mask on the wearer’s face).
The National Institute of Occupational Safety and Health (NIOSH) is responsible for conducting research and making recommendations for the prevention of work-related injury and illness and is a resource for information regarding healthcare and occupational PPE in setting on COVID-19. NIOSH also assesses important PPE to confirm efficacy and develops crisis strategies for coping with PPE shortages. NIOSH is responsible for the “N95” label on the mask you have likely been fit-tested to wear. The “95” generally indicates filtration efficacy of 95 percent of particles in the challenge aerosol (usually 0.1 micron diameter latex sphere aerosol) from the nose and mouth of the wearer. The “N” indicates that the respirator is NOT resistant to oil, “R” is somewhat resistant to oil, and “P” is oil-proof. (The oil resistance matters in some industrial settings in which the oils to which the respirator filters are exposed can remove the electrostatic charges from the filter media and thereby compromise filter efficacy.)
Fig. 1. Pictures of face masks under investigation. We tested 14 different face masks or alternatives and one mask (not shown). Photo Credit: Emma Fischer, Duke University.
In 2008, VanderSande et al. evaluated professional and homemade masks (made from tea cloth) for their efficacy in reducing respiratory infections in the general population and found that cloth masks provided a “modest degree” of protection to the wearer, while surgical masks were 25 times more effective and respirator masks were 50 times more effective at protecting the wearer than homemade cloth masks.1
S. Rengasamy et al., writing in Annals of Occupational Hygiene in 2010, analyzed filtration performance of cloth masks for particles 20-1000 nanometers in diameter and found instantaneous penetration level of 40 percent to 90 percent across the range of fabrics they tested.1
Fischer et al presented a low-cost technique for assessing filtration efficacy through various mask fabrics during speech and confirmed excellent filtration efficacy of respirator and surgical masks (figure 1), fair efficacy of some multilayered cotton, polyester, and mixed fabric masks, poor filtration efficacy with some cotton weaves as well as knitted masks and bandanas, and, somewhat remarkably, very poor filtration efficacy for fleece face coverings (often used in gaiters or “neck tubes”). (See figure 2) Fleece performed worse than no face covering at all, presumably by dispersing larger droplets into several smaller ones, thereby increasing the droplet count.
Davies et al., in Disaster Medicine and Public Health, tested the efficacy of homemade masks as protection in an influenza pandemic and offered that homemade masks should be used only “as a last resort” to prevent droplet transmission from infected individuals, but a homemade mask would be “better than no protection.”4
Scientists continue to study how and when and whom to mask since SARS and H1N1, and aerosol science will continue to evolve and to refine our use of PPE during and after the COVID-19 pandemic, but the overwhelming published scientific opinion supports the use of masks and, the better the mask, the better the protection for the wearer and those he or she faces.
Ready! Set! Mask!
References 1. VanderSande et al. 2008. PLOS ONE 3 (7) e2118.
2. S. Rengasamy et al. Annals of Occupational Hygiene, 2010. Vol 54, No 7, pp 789-798.
3. Fischer et al. Science Advances. SciAdv.10.1126/sciadv.abh3083, 2020.
4. Davies et al. Disaster Medicine and Public Health Preparedness. 2013 August: 7 (4) 413-418.
Kroger Health will offer drive-thru vaccinations noon to 6 p.m. Friday, Oct. 9 and 9 a.m.-3 p.m. Saturday, Oct. 10 in the Chevrolet parking lot at Dickies Arena, 3464 Trail Drive.
Kroger Health, the health care division of The Kroger Co., announced a partnership with the City of Fort Worth and Tarrant County as part of a comprehensive flu shot program designed to provide recommended vaccines amid the COVID-19 pandemic.
The Centers for Disease Control and Prevention estimates that during an average flu season, 8% of the U.S. population gets sick from the flu, with an average of 500,000 flu-related hospitalizations.
To make an appointment
If you do not speak English well, call the Tarrant County Public Health Information Line at 817-248-6299.
Si no habla inglés, por favor llame al Tarrant County Public Health línea de información a 817 248-6299.
Nếu quý vị không rành Tiếng Anh, xin vui lòng gọi đường dây thông tin Tarrant County Public Health (Y Tế Cộng Đồng Quan Tarrant) theo số 817 248-6299.
Walk-ups are welcome on Friday and Saturday.
Event details:
Flu shots will be provided at no cost, with or without insurance. Children must be six months or older.
Flu shots are available at no out-of-pocket cost to those with Medicare B and are also fully covered by many insurance plans. Bring identification and an insurance card.
For the safety of patients and the health care team, vaccinations are limited to one arm per vehicle door. Wear short sleeves.