Join us on Friday for our TCMS Physician COVID-19 Vaccine Event. In partnership with Tom Thumb/Albertson, we will be providing Moderna vaccines for TCMS members and their clinical staff who participate in direct patient care.
Members, if you did not receive the email or need additional information, contact Melody Briggs at mbriggs@tcms.org.
Tarrant County Medical Society is working with numerous pharmacies in Tarrant County to provide COVID-19 vaccines for physicians and their staff members.
The process will begin with allocations next week. We will provide details on scheduling appointments for you and your medical teams as soon as we have more information.
by Teresa Godbey, MD 2020 Gold-Headed Cane Recipient
This piece was originally published in the November/December issue of the Tarrant County Physician. You can read find the full magazine here.
Let me start and finish by saying “thank you.” Receiving the Gold-Headed Cane is a humbling experience for me, because I am not really a scientist, nor procedurally gifted, not an expert in any particular field of Medicine, have never published a scholarly article, and am not even currently on the front line of the SARS-CoV-2 pandemic. It’s been several years since I got out of bed to come to the hospital in the middle of the night, and even then it was often to call in the person who would do the procedure or make the decision that would be critical for our patients.
With a B.A. in English literature and a lot of courses in languages, I came late to the realization that I needed to apply to medical school. And I would not have done so had I not had a mother who was willing to keep an infant son so I could start all those math and science prerequisites, and a father who’d made it possible for her to be a stay-at-home mother and grandmother. So thanks to my wonderful parents. This decision to go into Medicine seemed to some like an abrupt change of pursuit, but for me, the unifying theme between my undergraduate studies and the practice of Medicine has been the privilege of learning people’s stories. In practicing Medicine, one can even help to bring about a plot twist or be a minor character in the story . . . but to hear what came before from disparate walks of life, then facilitate the ability of the patient to make their story unfold has been my motivation.
Some of those stories still make me smile years later. The patient who volunteered to run a small cemetery in a tiny town was at the cemetery when the grave for her mother, who had died at 103, was freshly dug. She met a young couple visiting in search of ancestral lore. In the process of helping them find a headstone of interest, she managed to back up and fall into her mother’s grave, sustaining a tib-fib fracture. Somehow, she managed to laugh at and see the mythic overtones of that painful experience. So many patients have shared their triumphs in life with me, with luck as well as gumption helping us all along the way. Sometimes luck is better than gumption. There was the decision to call a surgeon to see a middle-aged man, to remove a large obstructive right colon mass even though this mass, surely a malignancy, must have metastasized given its dimensions. The surgery was going to be diagnostic and palliative but proved curative when a plastic cocktail sword was found at the center of a large inflammatory mass.
Then there are the gut-wrenching stories of loss and the staggering abilities of some people to keep putting one foot in front of the other . . . the woman who witnessed one of her sons shoot and kill another. How she managed to grieve the loss of one of her boys, while still being a mother to the one who went to prison astounds me to this day. I can only hope that allowing her to relate this to me was in some way beneficial to her, but her strength and grace were such that I’m not sure I was needed.
It can be discouraging now to practice in an environment of corporate intrusion, such as to be told on which shelf the lubricant must be kept in the exam room, or to be coached to attest to diagnoses based on flimsy or inaccurate data. There are those of you who are gifted with a scalpel, a scope, a cath; those who can calm the chaos of the ER for a quiet moment to see a diagnosis coalesce. I suspect those abilities make it easier to keep a sense of purpose, so for those of us who are PCPs, let this be my plea. Hear the patient. Hear their story. See them. Feel them. There are times that I hear from a patient, “That doctor just came to the door, and never even examined me.” So yes, I know that current guidelines put ever less emphasis on certain parts of the physical exam, but please, keep honing your skills. The time spent on physical exam may not all be of value statistically. But when the unnecessary oral exam or rectal exam turns up a cancer, it changes your story as well as the patient’s. Plus, the patient who gets a rectal exam won’t tell someone else that you just came to the door. For those of us in primary care, using our senses is the only way we can, so to speak, change the ending.
And now, a few more people to thank: Dr. Stephen Eppstein, for driving from Fort Worth to Dallas on the one day of the week he could have relaxed a little, to be the town attending for my Internal Medicine rotation in 1984 . The town attending is the one you can ask the questions you might be embarrassed to ask your regular attending, like: Why aren’t there viral UTIs when there’s viral everything else? Dr. Kendra Belfi, the first female internist I really got to know, and who took such good care of my mother and my aunt. All the wonderful doctors in the Texas Club of Internists with whom I’ve enjoyed education and recreation over the years: thanks for waiting until the old guard died off so you could finally change the bylaws and let women in—in 1997. My son, Noah Boydston, for turning out mostly OK, and loving me even though I was away so much when he was little. Oh, and if you have to wait until age 48 to meet the love of your life, Leighton Clark was worth the wait. Thank you all.
Gold-Headed Cane Award Recipient Teresa Godbey, MD
By Allison Howard
This piece was originally published in the November/December issue of the Tarrant County Physician. You can read find the full magazine here.
If Teresa Godbey, MD, has one piece of advice for physicians early in their careers, it is to develop relationships with their colleagues. “Find at least one group where you want to go to meetings. You need other people. It’s fine to read and educate yourself on your own, but you need at least one regularly attended organized group.”
Dr. Godbey, TCMS’ 2020 Gold-Headed Cane Award recipient, is speaking from experience. In October, she retired after 33 years of practicing Internal Medicine in Fort Worth. Throughout her career, she has been a member of the Texas Club of Internists, the Texas Medical Association, and the Tarrant County Medical Society. “I don’t know what I would do without them.”
Though Dr. Godbey has long been involved in the medical community, becoming a physician was not her original plan. She got her undergraduate degree in English, but when she finished college, Dr. Godbey was unsure of her future career. She worked at Xerox for a year but soon realized that she wanted to go a completely different direction. Dr. Godbey was a new mother at the time, and she wanted stability and independence—and to do something that she loved. When she realized her interest and abilities converged at Medicine, she started down that path and never looked back. She began attending classes at UTA to get the necessary prerequisites to apply to medical school.
While the decision was sudden, the inspiration was not. Many people from her past influenced Dr. Godbey—from her beloved childhood pediatrician, Dr. Frank Cohen, to a favorite high school teacher, Valda “Frau C.” Carroll, who suffered from multiple sclerosis—these important individuals planted seeds that would impact her future. When the opportunity arose for Dr. Godbey to go back to school, her vision was clear: she was going to become a physician.
“Dr. Godbey has always been the type of physician I aspire to be myself. She has remained passionate about and fiercely committed to her patients, even in these times of increasingly heavy burden of clerical activities which constantly seek to burn us out and pull us away from the joy of direct patient care.”
Not everyone shared her enthusiasm. Between her young son and her English degree, Dr. Godbey’s academic counselor did not think she was a serious candidate for medical school. Dr. Godbey was told that she had to make A’s in all of her classes. “Thankfully, I was very confident then!” laughs Dr. Godbey. “That didn’t worry me.” No, she was not concerned about her math or science classes—it was PE that made her nervous. “PE was the class that really scared me. I intentionally got my undergraduate degree at a college that didn’t require it, but UTA was making me take PE. The only thing that would fit between the math and science courses and labs was racquetball. Racquetball!” Dr. Godbey remembers in dismay. Though racquetball was not her strong suit, her coach was fortunately more focused on dedication than ability. She completed all of her classes—even racquetball—with excellent grades and was accepted into medical school at UT Southwestern in 1980.
Dr. Godbey emphasizes that she did not go on this journey alone; she believes she never would have become a physician without the support of her mother. “She watched my son, Noah, for me. She loved it and made it possible for me to go back to school,” says Dr. Godbey. “I never could have done this without her.”
Once in medical school, Dr. Godbey began to consider the different specialties she could pursue. Everything came into focus during the beginning of her third-year rotations when she realized that she wanted to practice Internal Medicine. Dr. Godbey was originally considering a career as an OB/GYN, but when she recognized her love of interactions with patients during her medicine rotation and saw the appeal of building decades-spanning relationships with her patients, she shifted her focus, deciding to apply for a residency in Internal Medicine. She was accepted into Parkland Hospital’s residency program in 1984 and was hired by Internal Medicine Associates in 1987. She stayed with the group through mergers and acquisitions her entire career.
During her years in practice, Dr. Godbey developed the longstanding relationships she had hoped for with many of her patients. “My patients have aged with me for the most part,” she says. She also enjoyed the fact that primary care treats an expansive range of healthcare needs. While numerous patients and cases were significant throughout her career, one success comes to mind as a win she will never forget. A woman diagnosed with hyperemesis gravidarum had been sick in the hospital for weeks. She had been put on IVs and TPN, but as time went on, her condition continued to deteriorate. Numerous physicians had seen her, but they could not determine the root of the problem. When Dr. Godbey was called in, she looked at the chart and immediately saw something concerning. “I remembered Dr. Leonard Madison talking about beriberi when I was in medical school, which is thiamin deficiency. It was just there, on her chart. No thiamin.” At that time, there was a shortage of thiamin nationally, so it was not included in TPN. Since patients were generally not on TPN for an extended period of time it was not an issue, but because this woman had been using it for weeks, the deficiency was causing her significant distress. They quickly added an additional thiamin supplement to her IV, and within a day she had recovered and was on her way home. As much as it was an exciting experience for Dr. Godbey, she defers the credit to her medical school professor: “She got better thanks to Dr. Madison and his lecture on beriberi!”
“I don’t know of any doctor who deserves this award more. She is the most caring doctor I have ever known, always putting her patients’ needs and well-being above all else.”
Dr. Godbey’s colleagues emphasize that it is her complete dedication to patient care that characterizes her as a physician. Jennifer Arnouville, MD, says, “Dr. Godbey has always been the type of physician I aspire to be myself. She has remained passionate about and fiercely committed to her patients, even in these times of increasingly heavy burden of clerical activities which constantly seek to burn us out and pull us away from the joy of direct patient care.”
Over the years, Dr. Godbey certainly saw the practice of Medicine change, much as her own practice developed. What was once a group of seven or eight physicians has grown into what is now USMD, which is part of the even larger OptumCare. Though there were many adjustments, some things stayed the same. Ed Nelson, MD, one of the physicians who hired Dr. Godbey 33 years ago, continued with the practice alongside her. Dr. Nelson, Lee Forshay, MD, and Tom Davis, MD, were the partners at Internal Medicine Associates when Dr. Godbey joined the practice. She is grateful to have had the opportunity to work with these physicians; they helped shape who she is as a physician and her approach to patient care.
Reflecting back on when Dr. Godbey was hired, Dr. Nelson says the group could not have made a better choice. “What we couldn’t know then is what a great doctor she would be for the next 33 years. She and I have been associates, colleagues, and friends that whole time. I don’t know of any doctor who deserves this award more. She is the most caring doctor I have ever known, always putting her patients’ needs and well-being above all else.”
A number of physicians have supported Dr. Godbey throughout her career, including Stephen Eppstein, MD, and Roger Eppstein, MD; this father and son pair impacted Dr. Godbey in different but significant ways. Dr. Stephen Eppstein was her town attending in medical school, the person she could go to if she ever had a question or needed direction. “He was the safe one to ask for help,” she shares. He was also the one who directed her to Internal Medicine Associates. Dr. Roger Eppstein was one of her longtime partners at USMD. Dr. Nelson and Dr. Roger Eppstein were in her “pod” at the clinic and were often the physicians Dr. Godbey turned to for advice on difficult cases and to discuss new regulations or the state of Medicine. Even though she was in a large practice, the longstanding relationships she developed over time helped her overcome the isolation that can be a struggle in corporate medicine.
As she mentioned in her message to young physicians, Dr. Godbey believes that participating in organized medicine is an important part of connecting with fellow doctors and staying up to date on changes in the profession. “It’s a critical way to build relationships and meet people that can support you in your career that you can also support,” says Dr. Godbey. “I always know that TMA and TCMS are there for me—I would feel completely out of touch if I didn’t have the bulletins from TMA and Tarrant County Medical Society. New rules, new regulations, what’s happening currently with the pandemic. They keep me informed.”
Organized medicine also provides leadership opportunities and chances to break barriers, as Dr. Godbey experienced firsthand. When she was first considered for membership by the Texas Club of Internists, they required a 100 percent vote to add new members; because of this, a number of Internists, including minorities and females, were not accepted. Finally, in 1997, the Club amended their bylaws to fight these exclusionary practices. Dr. Godbey was the first female physician to attend a Club meeting, become a regular participant of the group, and ultimately, become the president; she served in that role in 2014. “It was amazing to see the how things changed—they barely let me in, and not 20 years later I was their president,” shares Dr. Godbey. She has seen other positive shifts over the years, such as rising numbers of female medical students. “It was 20 percent women when I went to medical school—now it is over 50 percent.”
While encouraged by the developments she has seen, Dr. Godbey believes that it is critical to continue advocating for minority and female physicians and any other groups that are not given full access to opportunities. Not just because doing so is best for individuals—it is also best for the practice of Medicine.
While advocacy and involvement are important, Dr. Godbey cautions young physicians to maintain work/life balance. Overall, she is encouraged by what she sees. “Younger doctors are better at prioritizing their homelife than we used to be,” she admits. “Don’t let go of that balance. Keep your interests outside of Medicine—reading, gardening, exercise. Whatever it is, it helps you keep your purpose in focus.”
When she in not busy Dr. Godbey enjoys hiking, cooking, and reading. Most of all, she loves to spend time with her family, including her husband, Leighton Clark, and their children. They have a blended family, which has added many blessings to Dr. Godbey’s life. “I had one son and I ended up with two sons and three daughters,” she shares. Between the two of them they have Noah, Philip, and Meredith; daughters-in-law Ashley and Mary; and granddaughters Marianne, Elinor, and Prudence. Dr. Godbey also shares a close relationship with her sister, Susan Pantle. Whenever possible, she and Leighton enjoy spending time with Susan and her husband, Mark.
Some things have come full circle; now that she is retired, Dr. Godbey and her husband will help watch their youngest grandchild, much as Dr. Godbey’s mother took care of Noah all those years ago when she was in medical school. “I’m excited to have the chance to give back,” says Dr. Godbey. “And to get to spend more time with Prue. I love taking care of my granddaughters.”
Dr. Godbey’s colleagues view her career as one hallmarked by commitment to her patients; her passion for excellence and empathy in providing care is something well known throughout Tarrant County’s medical community. “Dr. Godbey has been a role-model and mentor for me throughout the years that I’ve been in practice,” says Dr. Roger Eppstein. “Always a ‘doctor’s doctor,’ she has practiced evidence-based, compassionate Medicine throughout her career. It is no wonder why her patients have been so loyal to her. She has been practicing thoughtful ‘value-based medicine’ even before anyone coined this term.”
In acknowledgment of Dr. Godbey’s outstanding career, the Tarrant County Medical Society is proud to congratulate her as the 2020 Gold-Headed Cane Award recipient.
This piece was originally published in the September/October issue of the Tarrant County Physician. You can read find the full magazine here.
It happened twice in the same morning.
I saw two women for checkups that morning—their stories were so similar. Both older but not elderly, living alone, physically impaired needing a walker or motorized scooter, and always very crabby at their appointments. A litany of chronic non-specific complaints—fatigue, aching, headachey, etc. Honestly, I was not looking forward to their visits. They never seemed satisfied, and I never felt like I had helped them much. When I saw them both on the schedule that morning, I confess that I grimaced a bit.
But their telemedicine visits were just the opposite of their usual in-person visits. They both were happy, smiling, and relaxed. The conversations were easy and their questions were few. I anticipated much COVID-19 anxiety but found little; they were used to staying at home and hadn’t had to change their way of life much. They both just needed refills—I would have liked to have done a physical exam, but I really didn’t need to.
At the end of the morning, I wondered to myself what was different, and then it hit me. They didn’t have to physically come to see me, which so many of us take for granted but for them was likely a physically draining, frustrating, expensive, humiliating, and even painful experience. Wow. Was I humbled.
Telemedicine is a gift to some of our patients, such as parents stuck without childcare who have to bring multiple children along with them, people who lack reliable transportation, or elderly people who don’t like driving anymore but are embarrassed to ask for a ride. It can help someone two hours away who just needs a refill or a patient who can’t afford to miss work. I could go on and on; I’ve seen cases like every example I’ve given and I’m sure many of you have, too.
The coronavirus pandemic has added a new layer of urgency to the implementation of telemedicine. Physical distancing and shutdowns have made it extremely difficult, if not impossible, to see our patients safely face to face (especially when PPE is still hard to find). Telemedicine enables routine care to continue without the risk of exposure to the virus. It keeps medical offices safe and in business.
The AMA, along with many other organizations, has been developing telemedicine policy and recommendations for years. The AMA House of Delegates approved a report from the Council on Medical Services laying out principles for coverage and payment in June 2014.
An AMA survey in 2016 showed that 15 percent of physicians worked in a practice that utilized telemedicine in some way.1 But a far smaller percentage of actual patient encounters were done via telemedicine.
When COVID-19 struck and communities were shutting down all over the country, the telemedicine guidelines, reimbursement policies, and the work we had already done with CMS helped the organization be ready with their new guidelines for coverage and payment, which were initially released on March 17, 2020.
AMA had been working with the Physicians Foundation, the Texas Medical Association, the Florida Medical Association, and the Massachusetts Medical Society to create the Telehealth Initiative to provide a wide array of assistance for physicians to implement telemedicine in their practices.2 The launch of the program was not scheduled until later in the year but instead was moved up to March 19, 2020, just two days after the CMS announcement.
Virtually every medical society in the country now has guidance available for physicians on using telemedicine.
However, the current telemedicine coverage and payment program will only stay in effect as long as there is a national emergency, which has now been extended to the end of October 2020. Of course, we all know that COVID-19 will not be gone then, so AMA is working with state and specialty societies to lobby Congress for permanent solutions.
I believe that every specialty will develop its own guidelines for the appropriate use of telemedicine going forward, and every practice will utilize telemedicine to some degree.
The genie is out of the bottle. Let’s hope it stays that way. We deserve to be compensated fairly for services regardless of location, and our patients deserve the ease of access.
This piece was originally published in the September/October issue of the Tarrant County Physician. You can read find the full magazine here.
I was 13 years old the last time that I experienced a summer break, because it was that summer that I decided that I wanted to be a physician. I spent every summer after that through high school at the Volunteer Department of the nearest Level I Trauma Center in East Texas. If I wasn’t volunteering I was shadowing, and if I wasn’t shadowing I was scribing or taking classes that would prepare me for medical school. It became a constant cycle, month in and month out for 11 years. Every one of my spring breaks, winter breaks, and summer breaks was jam-packed with exciting new medical adventures, classes, or some other activity that was someday going to get me into medical school and ultimately help me become a physician. As crazy as it sounds, my story is not unique. This is the path for many students, former, current, and future, who pursue a career as physicians. This is a way of life that we gladly accept, because for many of us the idea of doing anything else is much more depressing than spending every break of our youth working towards our future career.
I was all geared up to spend the summer after my first year of medical school the same way. I had two in-hospital research projects lined up, was interviewing for a pediatric research program to review case studies and publish reports on the cases, and I was already looking for a summer job to bring in a little extra income during what I considered my “slow” month between the two academic years. Then, in an instant, a global pandemic hit, all my plans fell apart, and I was left with a very empty calendar during a period that was supposed to be a time for me to check all of the boxes that residency programs would want to see completed by the time I apply just three short years from now. When the initial shock wore off that a virus was capable of shutting down medical programs created and run by very people who live to combat these same types of diseases every day, it was like I had stepped into the sunshine for the first time in 11 years. As I began to read about the attempts of countries all over the world to contain and combat the virus, I was struck by an unexpected common theme in the rest of the world that I felt within myself: rejuvenation.
There were stories about nature being able to cleanse itself once people were no longer allowed to pour waste into it every day. Families were spending more time with one another at home, and smiles were being shared through technology all across the world because people were no longer able to go, go, go. Self-care began to emerge at the forefront of peoples’ minds, and I began to understand what it meant to take a step back and soak in the moments. I started cooking dinner every night, I read books on history and got outside every day. At a time when uncertainty was the norm and we were all scared, I spoke with colleagues and friends who were learning and growing personally outside the realm of medicine into better spouses, friends, and students. With this fresh new start that we received, we have been able to go back to school refreshed and ready to learn about medicine and people instead of being burned out and emotionally exhausted. During the time that our medical lives stood still, our mental and emotional health was able to re-blossom into excitement about life, medicine, and being the physicians that we are destined to become.
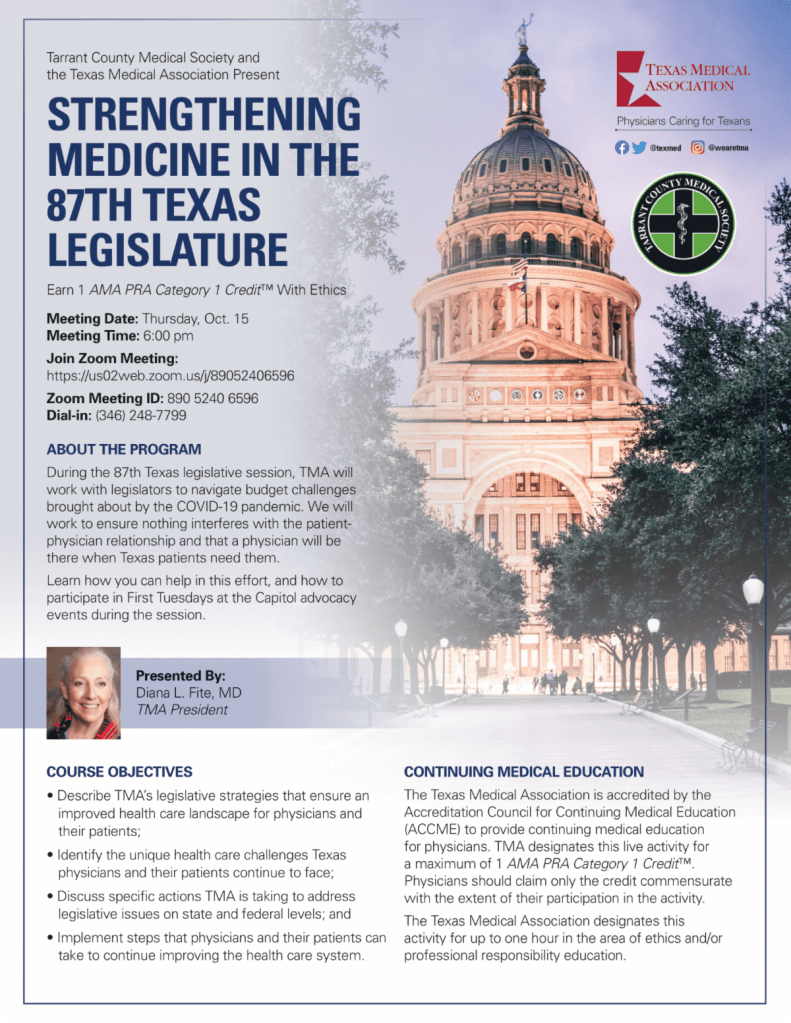
On Thursday, October 15, at 6pm, Tarrant County Medical Society and Texas Medical Association are presenting “Strengthening Medicine in the 87th Texas Legislature,” a virtual CME that will cover advocacy efforts that protect the practice of medicine and the patient-physician relationship.
The CME will be presented by TMA President Diana Fite, MD, and moderated by former TCMS President Robert Rogers, MD.
Early voting starts in Texas this week. Physicians urge all Texans to play it safe as they fulfill their civic duty, reminding everyone that it is possible to vote safely during a pandemic.
“Voting can be made safe by following the public health guidelines,” said Diana L. Fite, MD, president of the Texas Medical Association (TMA). “A little planning goes a long way.”
With the coronavirus still actively spreading in Texas, some elderly patients and Texans with disabilities wonder if it’s safe for them to vote in this year’s election, since they are most at risk for serious illness if they catch COVID-19.
Texans might have two options to vote: an individual might qualify to vote by mail, or he or she may vote in person.
“For those over 65 years old or who have chronic illnesses, it would be preferable to stay at home and send off an application for a mail-in ballot,” said Dr. Fite. “It’s certainly safer for these people to vote at home and mail their ballot than to venture out among crowds.” Any registered voter 65 years or older on Election Day or with a disability may vote early by mail in a Texas election.
The Texas Secretary of State has information and instructions about how to apply to vote by mail. Tip: The voter’s local voting clerk must receive an application for a mail-in ballot by Friday, Oct. 23.
For Texans opting to vote in person, there are options as well.
The early voting period runs Tuesday, Oct. 13 through Friday, Oct. 30. During this period, registered Texans can vote in person at any polling location in their home county. Voters might consider looking online for less-busy polling places and times, to avoid crowds.
Dr. Fite recommends early voting if possible to avoid any unforeseen problems. “If a person is sick on Election Day, that person should not go out to vote,” said Dr. Fite. “Instead, early voting is a consideration to avoid that possibility from occurring.”
On Election Day, Nov. 3, voters registered in a county that participates in the Countywide Polling Place Program may vote at any polling location in the county. If someone’s county does not participate in that program, he or she must vote in their own precinct on Election Day.
Whether voting early or on Election Day, physicians urge everyone to plan ahead and practice the same public health best practices as if they were going to the grocery store or anywhere else in public.
“Wash hands or use sanitizer before and after voting, try to stay 6 feet from others, and wear a mask,” said Dr. Fite. Simply maintaining space while waiting in line to vote can help prevent the spread of germs.
Physicians remind everyone of these tips for voting in person:
Stay at least six feet away from others;
Bring your own pen, pencil, or stylus;
Wash or disinfect your hands before and after voting;
Wear a face mask (you might have to remove it briefly for the election judge to confirm your identity); and
Stay home if you’re sick.
TMAis the largest state medical society in the nation, representing more than 53,000 physician and medical student members. It is located in Austin and has 110 component county medical societies around the state. TMA’s key objective since 1853 is to improve the health of all Texans.
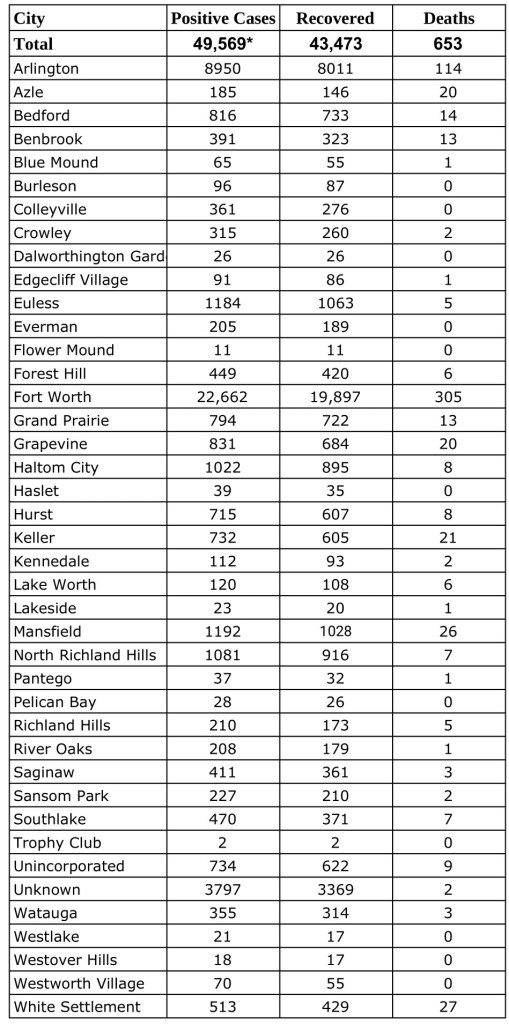
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Monday, September 28, 2020.Find more COVID-19 information from TCPH here.
* These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
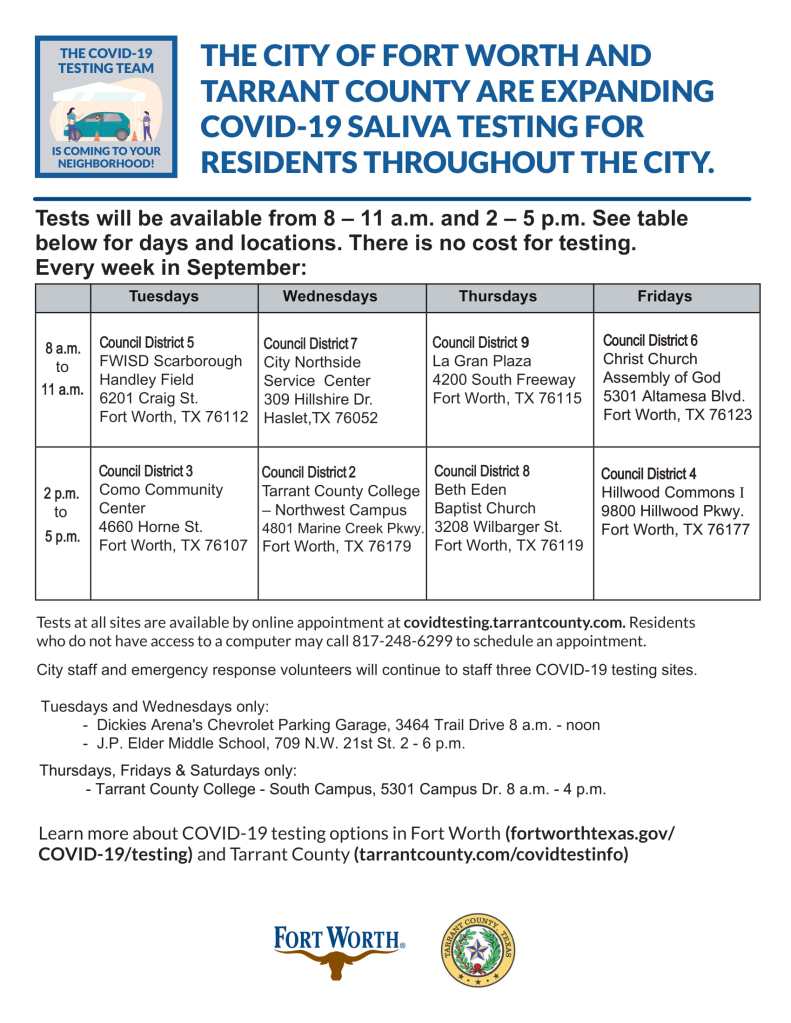
The below flyers provide information on COVID-19 testing that is being provided free of charge for residents of Tarrant County. The tests being offered are self-administered and saliva-based.