OFTEN ONE OF THE FIRST QUESTIONS I AM ASKED WHEN I mention that I am in medical school is, “How did you know you wanted to become a doctor?” Sometimes I scramble to find the most inspirational and motivating answer, as there were many reasons why I chose the career path that I did, However, at the core of every underlying reason was first, my love for science, and second, the desire to put that love into good use. Throughout my undergraduate years, I made sure to put scientific research at the forefront of my priorities. I took additional classes to help develop my skills as a researcher and participated in local symposiums whenever I could. Going into medical school, I kept research and the scientific process in mind as I learned about each body system. Given my medical education, I could delve further into the pathologies and the application of their respective treatments, and, if there were any developing treatments, I could keep an open mind about them and seek an opportunity to participate in the field research (if my busy school schedule let me). Thankfully, this past summer, my school presented the perfect chance to participate in the Pediatric Research Program (PRP) with Cook Children’s Hospital.
The PRP selects a group of second year medical students to take part in research “that aligns with their specialty interest.” There are also additional benefits such as being provided a mentor who guides you along the way and opportunities to present work at local/regional/national conferences. I chose neurology as y number one field of interest, so I was assigned a case study with a pediatric neurologist as my research mentor. I was excited and eager at the prospect of beginning work, especially since I had been assigned to Cook Children’s. The idea of being in an environment that was dedicated to helping children with challenging diseases brought a sense of fulfillment to my foundational goal of helping people heal.
Writing a case study was a novel experience, but I was fortunate to have a dedicated mentor who aided me through the process and helped me understand clinical information that my then year-one-medical-student mind could not comprehend. My mentor further allowed me to shadow her periodically throughout the summer, which was a nourishing experience to my medical education. I was able to interact with many pediatric patients who were affected by a variety of neurological disorders, especially congenital ones. This provided me with an appreciation for specialist physicians since they offer a great sense of hope and security to their patients- something I had associated more with primary care. What was even more admirable was my own mentor pursuing her research and developing case studies to help spread awareness of the pathologies that affect her patients.
Regarding my own project, I was able to learn more about the neurovascular complications of Marfan syndrome and the importance of considering it as a possible cause of stroke. I thoroughly enjoyed the process of gathering information and researching literature since it showed me how physicians from different parts of the country can come together and use their scientific nature to bring light to issues and possibly come to solutions. I look forward to working on more case studies and research projects as a medical student because it reaffirms my belief in using scientific methods and research to better the lives of patients and reach new heights in treatments.
by Catherine Colquitt, MD, AAHIVS Medical Director and Local Health Authority Kenton K. Murthy, DO, MD, MPH, AAHIVS Assistant Medical Director and Deputy Local Health Authority
During the holiday season, many were reunited in person to celebrate with loved ones after almost three years of relative seclusion.
There was much to be grateful for this season. While COVID-19 case counts and hospitalizations are rising in Texas and in Tarrant County, our present COVID rates pale in comparison to December 2020 or January 2021.1 And though influenza and Respiratory Syncytial Virus (RSV) infections are strikingly and unseasonably high, and the perils of a tridemic (COVID-19, influenza, and RSV) are on our minds, many of us and our patients and neighbors are fully vaccinated against COVID-19 and have already had the bivalent mRNA vaccines (for protection from the Wuhan and Omicron COVID-19 strains) as well as the current seasonal influenza vaccine.
As we shift gears from the COVID-19 pandemic to COVID-19 endemic, we hope that our next iteration of COVID-19 vaccines will roll out side by side with next season’s influenza vaccine. However, if new versions of COVID-19 vaccines are required to mitigate the spread of COVID-19 between now and then, our scientists and vaccine manufacturers, our distribution networks, the FDA, the Advisory Committee on Immunization Practices, the CDC, and state and local partners will work together to respond to future challenges.
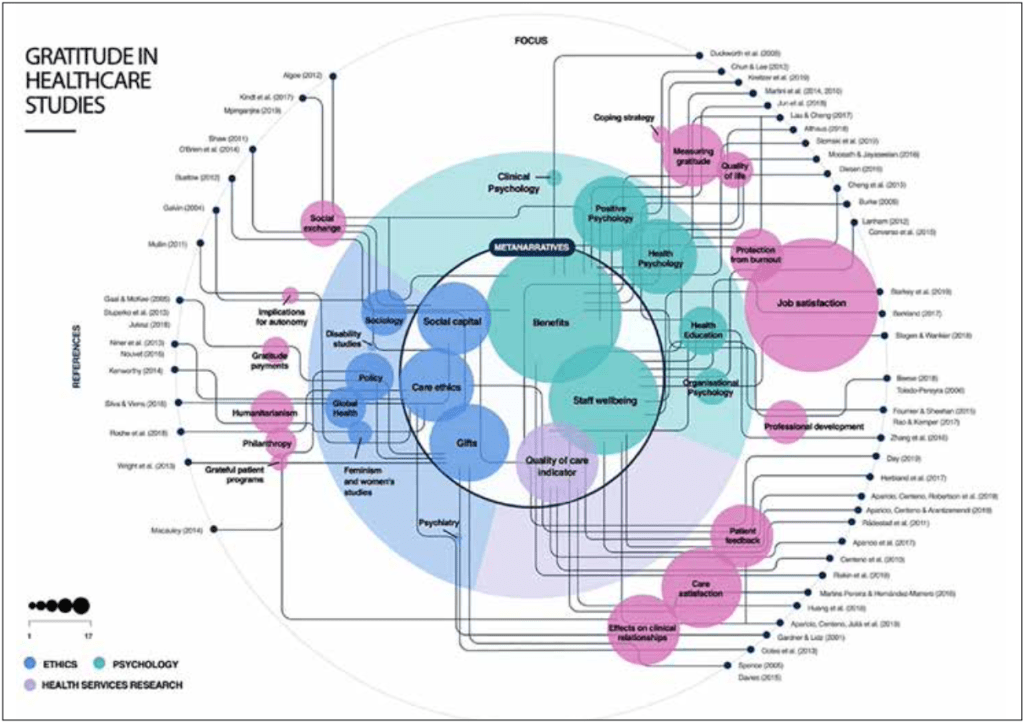
It seems fitting to consider what we have to be thankful for, and gratitude in healthcare is a very active field of study at present. A meta-review in Qualitative Health Research by Day et al reviewed recent works and referenced pioneering works on gratitude research dating to the early twentieth century and organized this vast body of work into six “meta- narratives: gratitude as social capital, gifts, care ethics, benefits of gratitude, gratitude and staff well-being, and gratitude as an indicator of quality of care.”2
Given the ubiquitous articles reporting on healthcare worker burnout and the mental and physical consequences of COVID-19 on our workforce, Day et al suggested in their conclusion that more research is needed on “gratitude as a component of civility in care settings” and that further study might help researchers to understand the intersection of gratitude “with issues of esteem, community cohesion, and the languages of valorization that often accompany expressions of gratitude.”2
Individually, we might all take a moment to self-assess using a simple exercise such as the Gratitude Questionnaire – Six Item Form (GQ-6), or we might dig more deeply into the bibliography of “Gratitude in Health Care: A Meta-narrative Review” to study our own complicated relationship with gratitude more closely.2,3 Those in healthcare have been under great strain since COVID-19 first appeared on the scene, and perhaps a gratitude practice is just what the doctor ordered to help us to reboot and revive the sense of wonderment with which we began our careers.
References 1. Texas Department of State Health Services COVID -19 Dashboard. 2. Giskin Day, Glenn Robert, Anne Marie Rafferty. 2020 Gratitude in Health Care: A Meta-narrative Review. Qualitative Health Research. 2020 Dec; 30(14): 2303-2315 3. Gratitude Questionnaire – Six Item Form (GQ-6), taken from Nurturing Wellness by Dr. Kathy Anderson.
When Dr. Gregory Phillips starts seeing patients for the day, it isn’t in his office, as you might expect for an internist. No—he begins by making rounds at Texas Health Harris Methodist and HCA Medical City hospitals, checking up on any of his patients who are currently admitted.
“I am usually at the hospital, I don’t know, 6:00, 6:30?” Dr. Phillips says. “And then I usually get to my office at 8:00.”
Going to see his patients in the hospital makes Dr. Phillips a bit of a unicorn in the medical world; the red tape of credentialing complications and readily available hospitalists have made the practice nearly obsolete. But Dr. Phillips has seen admitted patients throughout his over 40 years of practicing medicine in Fort Worth, and it means the world to them.
“I saw a 94-year-old lady in the office today with her daughter, and I said, ‘What was your good experience and bad experience with your hospitalization at Harris?’’ says Dr. Robert Keller, who works with Dr. Phillips at his private practice, Fort Worth Medical Specialists. “And they said, ‘Dr. Phillips showed up every day at the same time, and we could ask all of our questions and he knew all of the answers.’”
Dr. Keller, who spent years as Dr. Phillips’ call partner before joining his practice in 2021, pauses to reflect as he recalls the conversation. “That’s a classic story for Greg. He is devoted to his patients . . . I call it ‘covenantal care.’ His contract with his patients is not simply economic, it’s not simply medicine – it’s covenantal. You’re in this together.”
But Dr. Phillips’ commitment to medicine and the community extends beyond his own practice. Throughout his career he has been dedicated to organized medicine, educating medical students, supporting the arts, and advocating for the underserved of our community. And, yes, his patients.
That is why Dr. Phillips’ colleagues are recognizing him as the 2022 Tarrant County Medical Society Gold-Headed Cane recipient, an honor that is given to the “Doctor’s Doctor” for their excellence in patient care and impact on the practice of medicine in Tarrant County.
“Dr. Phillips is a ‘Doctor’s Doctor,’” says his friend and fellow physician Dr. David Donahue. “Colleagues consult him for care and counsel. Dr. Phillips’ possession of the golden cane represents a credit to his fellow physicians and is a justifiable tribute to him. The award takes on a new significance. We congratulate him.”
______
For Dr. Phillips, becoming a physician wasn’t inspired by a single moment or person. You might say it is part of his nature – because if you ask him, it was always a defining part of his life.
“I can remember from my earliest days,” he says.
“You know, people ask you what you want to be, and I think I always said I wanted to be a doctor. I’ve never really thought of anything else. And if I weren’t a doctor, I honestly don’t know what I’d be doing.”
Perhaps it isn’t surprising – his family has a strong medical background. His father was a dentist, his mother a nurse, and his two uncles and grandfather were doctors. Dr. Phillips likes to joke that his lifelong commitment to medicine took a weight off of his five younger siblings and their cousins.
“Once I said I’d be the doctor, no one else had to do that,” he says, laughing. “I was going to be the doctor out of our generation. They were all free to do whatever they wanted.”
Dr. Phillips never wavered from his vision and began his journey to becoming a physician in Fort Worth shortly after graduating from high school – but he didn’t necessarily plan to stay here.
“I never thought I’d be spending my life in Texas,” he says. “I think of myself as a West Coast kind of guy.”
After graduating Summa Cum Laude with a degree in biology from Texas Wesleyan University in 1970, he attended medical school at UT Southwestern in Dallas, and completed his residency in internal medicine at the St. Louis University Medical School in Missouri. It was when he began a fellowship in clinical nutrition at the University of California Davis that Dr. Phillips hit a bump in the road.
“I went to California, thinking I would take this fellowship and stay in academics, but the state of California ran out of money in 1978; as a result, the medical school eliminated the entire clinical nutrition program,” says Dr. Phillips. “I found a job in Fort Worth that year in 1979, and I’ve been here ever since.”
Though he has been in private practice since coming back to Texas, Dr. Phillips has still been involved in the educational side of medicine through Tarrant County’s two local medical schools—he is an adjunct clinical professor of medicine at the Texas College of Osteopathic Medicine at UNT and an assistant professor of internal medicine at the Anne Burnett Marion School of Medicine at TCU.
Though it was a deviation from his original academic plans, Dr. Phillips has found his work as in internist incredibly rewarding. Throughout his career he has built a thriving practice that has fostered long-term relationships with patients and given him ample opportunity to exercise his passion for nutrition and preventative healthcare.
“I didn’t even know what internal medicine was when I started medical school,” says Dr. Phillips. “I knew I wanted to be a doctor and had spent summers working as a surgical orderly here in Fort Worth at one of the hospitals, so I knew that I didn’t want anything to do with surgery. So then, when you go through training in medical school, you realize that there’s this whole specialty called ‘internal medicine.’ You don’t do operations, you don’t deliver babies, you don’t see kids. It’s all adult primary care medicine. Once I realized that was an actual specialty, that was what I decided that I wanted to do.”
Dr. Phillips smiles. “It’s almost like they made that specialty just for me.”
______
While he impacts the Tarrant County community every day by caring for his patients, Dr. Phillips’ dedicated involvement in organized medicine gives him a much broader reach. Beyond his TMA and TCMS membership, he is a member of the American Heart Association, American College of Physicians, National Lipid Association, and the Association of Black Cardiologists (ABC).
“My friend who was presenting about the ABC at a meeting was saying, ‘If you care for minority and underrepresented populations, you should join our organization,’” Dr. Phillips explains, noting that it might seem odd that he is a member of the Association of Black Cardiologists when he is neither Black nor a cardiologist. “But Dr. Ferdinand said, ‘You don’t have to be a cardiologist; you don’t even have to be Black. You can join our organization.’”
So that’s what Dr. Phillips did.
“It’s just one example of getting involved with an organization that has part of its mission to see what it can do to help healthcare for disadvantaged, disenfranchised populations,” he says.
Throughout his work in organized medicine, Dr. Phillips has served in numerous roles, including as our 2016 TCMS president and as a Project Access volunteer. He has sat on many boards and committees, including the Board of Directors for the American College of Physicians Texas Chapter, the Southwest Lipid Association, and the Recovery Resource Council.
Eric Niedermayer, CEO of the Recovery Resource Council, says that Dr. Phillips has had a tremendous impact on the organization, which is focused on fostering wellness and recovery for those struggling with addiction and trauma.
“[Dr. Phillips] has truly given of his time, talents, and resources every year,” he says. “During the summer of 2022, he helped the Council’s Overdose response team obtain $100,000 of Narcan to distribute to survivors of fentanyl and other opioid overdoses by providing the necessary authorization for this life-saving intervention . . . To me, he is a person I can count on to do whatever he can whenever he is asked to help. That makes him a rare find for any non-profit that is always faced with new challenges or opportunities.”
He uses the same approach for each organization he has joined – if he is going to be a member, he is going to be involved. This is what eventually led to one of his career highlights: from 1990 to 1991, he served as the president of the Texas Affiliate of the American Heart Association, and he was then appointed to the American Heart Association’s National Board of Directors from 1993 to 1995.
“So this little kind of average internal medicine doctor from Fort Worth would have no business there,” says Dr. Phillips. “I don’t do research; I don’t write grants. I’m not the chairman at the department of a famous medical school. But I’m at these meetings with all of these famous people. And it’s because I demonstrated a commitment to the mission of the organization and showed that I participate and help whatever needs to be helped.”
______
While medicine is certainly a passion for Dr. Phillips, it isn’t the cap on his interests. He loves supporting the arts and is especially involved in sponsoring local efforts. He is a patron of both the Circle Theatre and Bruce Wood Dance.
“It’s also been very rewarding because I’m not in any way an artistically talented person, but being able to work with the theater group or the dance company . . . to support their work with both time and money, is something that I’ve been able to do,” Dr. Phillips says.
He has also been an active member of Texas Wesleyan University’s Board of Trustees for over ten years, and he is currently serving on their Executive Committee. Much like his interest in the arts, Dr. Phillips views this as a way to broadly make an impact for good through the value his alma mater brings to its students and the greater Fort Worth community. Dr. Tom Cockerell, his former neighbor and longtime friend, says that civic involvement has always been a priority for Dr. Phillips, alongside his work in medicine.
“Through the years Greg has been able to continually balance a busy practice with family and civic and professional leadership demands at the local and national level,” says Dr. Cockerell. “Anyone who knows Greg admires his amiable nature, his recognition of and loyalty to important enterprises, and his good sense.”
Though he says his hobby is going to meetings, Dr. Phillips also enjoys playing golf when he has the chance. But between his practice and the different groups he is involved in, he always makes time for his family.
“I save my time off to go be with them,” says Dr. Phillips.
Whether it’s visiting his son, Lauren, in Lubbock; or his daughter, Karen, her spouse, Kyle, and his two grandchildren, Elodie and Ezra, in Santa Fe; getting to spend time with them is the highlight of his year.
As Dr. Phillips looks to the future, two things are very clear to him: he wants to keep practicing medicine and fighting for equity.
“I don’t have a plan to retire,” he says. “And I do think that people in the profession who do have time and financial resources and influence to try bringing the whole population up is something to try to focus on. I don’t know exactly where I fit into that whole puzzle, but I hope that during the rest of my career that can be one of the priorities that I have – to continue working on improving the healthcare of people who have been disadvantaged for so long.”
It is Dr. Phillips’ legacy of driven yet compassionate care for the patients of Tarrant County that has led his colleagues to recognize him as the 2022 Gold-Headed Cane recipient. With much appreciation for his service, past, present, and future, we congratulate Dr. Phillips as “the Doctor’s Doctor.”
Dr. Combs giving her first speech as the 2022 TCMS president
And just like that, my year as the Tarrant County Medical Society president is nearly over. It has been a pleasure to serve in this role, and while my time is almost up, I wanted to look back over the past year.
My time started at the end of last year during an early reprieve from the COVID pandemic. The Gold-Headed Cane and President Installation was our first in-person event since the start of COVID. It was an amazing night of getting to see old colleagues and meet new ones. It was also amazing to have four female physicians being honored in one night; it was great to share the evening’s celebration with Drs. Susan Bailey, Teresa Godbey, and Angela Self.
Being inducted by Dr. Angela Self as the new TCMS president
Unfortunately, the year took a step back due to the COVID pandemic, and we once again had to change to a virtual meeting for the TMA Winter Conference. As we have done multiple times during the pandemic, we were able to pivot and carry on. Locally, our TCMS leadership came together to promote fellow physicians to seek out positions at TMA.
As we moved to April, we started to see light and were finally able to hold TexMed in person, the first time since 2019. The best part of the meeting was seeing the inauguration of our own Gary Floyd as TMA president. Moving into summer, we were able to have a Women in Medicine event where we gathered for some much-needed stress relief making bath bombs. While we were not all successful at making the bath bombs, we had a great time gathering again in person.
Making bath bombs at the Women in Medicine event
When the Dobbs decision came out in June, I had multiple opportunities to speak with local and national media about the importance of the patient/physician relationship, and how this decision has many far-reaching implications in medicine. I will continue to work on advocating for doctors and patients to make their own medical decisions without intervention from outside forces.
At the Young Physicians Mixer
During July, I had the privilege to welcome our new Tarrant County medical students from the Texas College of Osteopathic Medicine and the Anne Burnett School of Medicine at TCU to TCMS and the world of organized medicine. It was refreshing to meet with these young students and to cheer them on as they begin their journey to having the greatest job on the planet: being a physician.
As we moved into the fall, we had another opportunity to gather again at the TMA Fall Conference. We are slowly finding our way through this COVID pandemic, returning to some form of normalcy. While I cannot quite say it seems to be over, as this has been said too many times before, we continue to find a way through.
Speaking to the incoming class of medical students
While my tenure as TCMS president may be coming to an end, I will continue to contribute to the work of our county, state, and national medical societies. If I have learned anything over the past year, it is that we must be at the table and part of the discussion; otherwise, people who don’t practice medicine will continue to try to tell us how to do our job. We have worked too hard to become physicians to allow others to practice medicine for us, and it isn’t in the best interest of our patients or our vocation – the work that still is, despite so many challenges, the best job on the planet.
This article was originally published in the July/August2022 issue of the Tarrant County Physician.
As medical students, we have an incredible opportunityto discover a vast amount of medical knowledge, learn about the normal and the pathological, and to immerse ourselves in clinical settings where we witness the complexity of diseases. In the process of learning about life-threatening diseases, the risk of nosophobia, or illness anxiety disorder, can develop. More commonly termed “Medical Student Syndrome,” it is a concept that medical trainees are well acquainted with.
What is Medical Student Syndrome? It is the phenomenon that causes fear of contracting or experiencing symptoms of the disease that the students are studying or are exposed to.
Medical students learn the pathophysiology, the diagnosis, the treatment, the prognosis, the best-case scenario, and the worst-case scenario of diseases. We learn about teenagers diagnosed with melanoma and hear stories about patients in their early 20s diagnosed with breast or cervical cancer. The worst-case scenario tends to grab our attention. This reinforces us to not ignore a patient or symptom that doesn’t follow the general pattern of the disease, allowing us to widen our baseline scope of clinical suspicion when it comes to debilitating pathologies. The constant medical stimulation and limited clinical experience earlier on in our education can cause students to become preoccupied with symptoms and construct connections between what we are experiencing with the worse-case scenarios we learn about.
“I booked an appointment with the dermatologist because I thought I had a melanoma,” said one classmate after we shortly finished our dermatology unit. After undergoing a biopsy, the classmate discovered that the melanoma in question was a benign nevus. During the cardiopulmonary block, another medical student said he went to the ER after experiencing mild epigastric pain and tachycardia, thinking he was experiencing symptoms of atypical myocardial infarction. He had recently encountered a patient in his late 30s with a history of MI who presented with similar symptoms, further reinforcing the “worst-case scenario” in this trainee’s mind. After hours spent in the ER, he was diagnosed with gastritis and sent home with a prescription for a proton-pump inhibitor.
Throughout my medical training, I have heard countless stories resembling these. This is not an uncommon phenomenon that trainees experience. It is a topic that everyone in medicine is familiar with, whether through personal anecdotes or through stories discussed with classmates, mentors, and acquaintances. Understanding the complexity of medicine takes more than four years of medical school. Medicine is a field that requires life-long learning and an internal motivation to be updated with evidence-based practice. Expertise comes with clinical experience and after encountering numerous successes and failures. I believe that these experiences can help future physicians connect with their patients more effectively. If we as medical trainees can fall victim to an overwhelming fear of vague symptoms, how can we expect our patients with limited medical knowledge to be immune to this? With Dr. Google, a benign tension headache can be escalated to look like brain cancer. Understanding these fears and reflecting on the days when we experienced these uncertainties can bridge the gap in patient-physician encounters. It allows us to effectively address the patient’s fears without judgement, urging us to educate our patients about their symptoms instead of dismissing or minimizing them.
This article was originally published in the September/October 2022 issue of the Tarrant County Physician. You can read find the full magazine here.
Over the past year, the Texas Medical Association has had to weigh in on one sensitivetopic after another—from issues impacting the patient-physician relationship to how physicians practice medicine and the prevention of further cuts in the Medicare program.
Often, after TMA publishes its stance in the association’s daily newsletter, Texas Medicine Today, we receive inquiries from members on how TMA came up with that position since no one surveyed them individually or asked for their opinion. This has made me realize many of our members don’t understand who runs TMA or the process TMA uses to develop its policy, which drives the association’s communications and advocacy.
The association is governed by a 500-member House of Delegates, the legislative and policymaking body. The House is made up of elected county medical society delegates (one delegate per 100 members or fraction thereof) and the following ex officio members: members of the Board of Trustees; 15 councilors; Texas delegates and alternate delegates to the American Medical Association; members of the Council on Legislation and chairs of the other councils; delegates from the Young Physician Section, International Medical Graduate Section, Resident and Fellow Section, Women Physician Section, LGBTQ Section, and Medical Student Section; and delegates of selected specialty societies.
The House of Delegates meets every year at an annual session held during TexMed in the spring. In 2023, TexMed will be in Fort Worth on May 19–20.
The best way to get your idea adopted as TMA policy is to begin at the grassroots level.
1 Present your idea or change to an existing policy at your county medical society meeting. Ideas and actions also are developed by association boards, councils, committees, and sections. You can work with these groups to develop a policy recommendation.
2 If the county society, section, or other entity agrees, it can submit your idea as a report or resolution to be considered at the next meeting of the House of Delegates. Instructions for writing a resolution are at http://www.texmed.org/Resolution.
3 Every report and resolution is assigned to a reference committee that vets it further through open hearings at which any TMA member can testify. The reference committees then send their recommendations on each report and resolution to the house. If you would like to serve on a reference committee, let our House of Delegates speakers know by filling out the form at tma.tips/refcom.
4 If your idea is adopted by the house, it is incorporated into the TMA Policy Compendium (www.texmed.org/Policy). If it has nationwide appeal, it may also be forwarded to AMA for action.
As TMA president, I am obliged to represent our TMA policies. As you can imagine, we have members on both sides of several very sensitive issues. Some members would like TMA to issue an immediate, strong opinion favoring their stance. However, by working with our legislators, we have learned that calm, measured, commonsense approaches are far better received than knee-jerk responses. Therefore, in our responses we tend to emphasize areas of commonality for our members, like protecting the sanctity and privacy of our patient-physician relationships and creating a safe environment for our physicians to exercise their best medical judgment in providing the appropriate standard of care for all their patients.
Please reach out to your county medical society and learn more about TMA’s policymaking process. We want to hear from you!
This article was originally published in the September/October 2022 issue of the Tarrant County Physician. You can read find the full magazine here.
On June 23, 2022, the Tarrant County medical community lost an amazing physician, who died by suicide. He was a remarkable person whose work touched so many lives—he was always willing to help others. He is greatly missed by all who knew him.
Unfortunately, physician suicide has become an all-too-common occurrence in the United States.
• Approximately 300–400 physicians die by suicide each year in the U.S.
• Among male physicians, the suicide rate is 1.41 times higher than the general male population.
• Among female physicians, it is even more pronounced at 2.27 times higher than the general female population.1
As terrible as this sounds, there is hope. Physicians who are proactive about their mental health are able to take better care of their patients as well as have more resilience in the face of stress. However, this is not so easy to accomplish.
There is already a stigma associated with mental health, and it is made even worse for physicians due to the concern of needing to report a diagnosis to our medical boards, licensing organizations, as well as to credentialing offices in the hospitals and health systems we work in. We as physicians also have difficulty taking care of ourselves in general, let alone when it comes to mental health, as we are the healers and must be perfect.
The truth is, being a physician is hard. We train for many years to be able to do the work that we do. We often share our war stories about medical school and residency, but when it comes to the deeper struggles we have, we tend to keep those to ourselves. We push them down and hide behind a smile (or a mask) and continue to pretend that everything is okay.
But it’s not okay.
We as a profession need to start taking care of ourselves and looking out for our colleagues. It is okay to tell someone when you are struggling and to seek out help when you need it. A psychiatrist friend puts it best—“Everyone needs a therapist. I have one.” At some point we all learned the physiology of the human body, and of the brain specifically. Sometimes that brain needs a little extra help from chemistry, and that is okay as well. If you have a thyroid problem, you do not put up a fight about taking a thyroid pill. The same goes when our brain chemistry needs a little help. We also need to reach out to one another, to check in and see if our colleagues are really doing okay and if they need any help or support. It’s okay to not be okay, but we need to recognize this and seek out the help we so desperately need, and to help our colleagues obtain the help that they need.
We also need to work from an advocacy standpoint so that physicians can seek the help that they need without the fear of needing to report their illness. All other aspects of medicine and healthcare are taken care of in a private manner between a physician and a patient. Why should mental health be any different? Until this changes, no number of wellness programs, resilience building, etc., will be able to fix the problem.
I encourage everyone to seek help when needed and to reach out to our colleagues, partners, and friends. We have worked tirelessly to get to the point we can practice medicine, and those around you want you to stay here.
References 1John Matheson, “Physician Suicide.” American College of Emergency Physicians. Accessed August 3, 2022.
National Suicide Prevention Lifeline 1-800-273-TALK (8255) Available 24/7
Crisis Text Line Text TALK to 741-741 Available 24/7
Physician Support Line 1 (888) 409-0141 Open seven days a week, 7:00am – 12:00am CST Psychiatrists helping their U.S. physician colleagues and medical students navigate the many intersections of our personal and professional lives. Free and confidential. No appointment necessary.
Emotional PPE Project emotionalppe.org The Project connects healthcare workers in need with licensed mental health professionals who can help.
This article was originally published in the September/October 2022 issue of the Tarrant County Physician. You can read find the full magazine here.
The first time I saw and treatedpatients in a private practice setting, other than moonlighting in an ER or at the Cook County jail, was in 1968 when my dad, a general practitioner, had a heart attack as he entered Oak Park Hospital to make rounds on a freezing January day. He checked himself into the ER, ordered an EKG, and later called me from the ICU to ask if I could cover his office appointments once or twice a week. My mother, who knew all of his patients, called and rescheduled appointments for the evenings when I was free from my third-year orthopedic resident responsibilities.
I dressed in a suit and tie, removed the blood stains from my shoes, and carefully combed my hair. Not the usual resident attire; I had to look dignified to fulfill this responsibility. The first night, elderly Mrs. Novak came for her office visit with a simple request for cough syrup, adding a weak, pitiful “cough, cough.” I wrote a script which she promptly handed back, “No, no. that’s not the right one,” she admonished. “The one with the silver label, the one your dad gives me. I think the name is, oh, I don’t remember. I wrote it down so there’d be no mistake.” Knowing exactly what she was seeking, she handed me the note. I looked up the medicine’s name in the PDR (an old-fashioned, remarkably thick and heavy red book with Bible thin pages listing every known medicine in three separate indexes in a way only Sherlock or an egghead could understand). Carefully perusing the ingredients, I saw: 15% alcohol. Over the next few weeks, I got several more requests for medicinal nightcaps.
The second evening a patient reported, “I’ve got my usual sinus infection again, and I need the treatment your dad does. It’s the only thing that works.” I nodded knowingly and said, “Just a minute while I get some extra supplies.” My dad shared this office, a converted residential apartment, with a friend who was a dentist. My dad’s part was the dining room and kitchen, while Ed drilled teeth in the bedroom and made crowns in a closet. They were like two peas in a pod. I stepped into Ed’s closet and, despite my dad still being in the ICU and after much hesitation, called the Oak Park Hospital where a dedicated nun answered, “Okay, I can let you talk to him this time, but we can’t make a habit of it.” Hah, little did she know.
I got carefully worded instructions as to what “the treatment” was. After wrapping a generous wad of cotton on an applicator, I soaked it in epinephrine and then in cocaine (standard office formulary at that time). Next was the hard part, a part my dad had extensively practiced but I had never conceived of doing. I put on the doctor’s head mirror, the kind you used to see doctors wear in cigarette commercials, and sat facing the patient, who was in a chair in front of a bare lightbulb. I tried to look professional and adept at peeking through the hole in the center of the mirror while focusing on the patient’s nose, but I blinded him with the concentrated glare. Since my retina-burned patient squeezed his eyes shut and couldn’t see my incompetence, I felt comfortable peeking around the mirror’s edge. I jammed and twirled the cotton swab quickly into one nostril, then the other, pausing to wipe away the tears, his and mine. Seeing no blood, I surmised I hadn’t done much damage. After a burst of sneezing and snorting, the patient said, “Thanks, doc, that’s a whole lot better already,” as he blew more stuff out than I cared to look at.
My dad’s carefully worded instructions included, “I usually charge ten dollars, but his wife recently fractured her ankle, and they have more medical bills than they can afford. So charge him three dollars total.” The instructions didn’t end there. “I know what you’re thinking so listen, I decided long ago that for my peace of mind I would maintain my independence. I choose to run my business as I see fit, believing that if I take care of my patients, they will take care of me. They’re our neighbors, not cash registers.”
Okay, lesson received. But the execution turned out to be the tricky part. He came ready to pay more, so he handed me a twenty-dollar bill. Oh goodness, the change must be seventeen. I, too, had come prepared: five- and ten-dollar bills together in my right side suitcoat pocket, and a roll of ones on the left. Being a bank teller couldn’t be that hard—after all, I went to medical school. I took his twenty with my left hand and reached into my right suitcoat pocket for the carefully divided packet of larger bills. I set the twenty on the desk so I could select one five and one ten from the bundle, and put the rest back in the right pocket, while retrieving the one-dollar bills from the left pocket. Holding the fifteen dollars pinched between my little finger and palm, I tried to count two singles, but when they stuck together, I dropped the whole wad of ones on the floor. Scrambling like a pigeon chasing crumbs was ultimately undignified regardless of how impeccably I was dressed.
Then came Mrs. Smith. Mrs. Smith’s young daughter had a skin condition (my worst subject was dermatology, which in my mind is akin to sorcery), and Mrs. Smith wanted the cream my dad had prescribed last time. Once again, I had no idea what she was talking about. I searched and searched for Mrs. Smith’s record and found nothing on her, her husband, or their daughter. In fact, there was only one Smith in the entire file; it was a most uncommon name in that neighborhood. I gave up and called the same dedicated nun, who reluctantly turned the phone over to my dad. “Where is Mrs. Smith’s chart? She wants the cream for her daughter’s rash,” I asked. My dad chuckled, then said, “Look on the chart labeled ‘Prochaska.’ Lillian Prochaska is Lorain Smith’s mother, and all the family’s records are on one chart.” Even Mrs. Smith’s husband and daughter? It almost blew my mind. I recovered the Prochaska family “chart,” three five by eight index cards stapled together, a system from the 1930s when he built his private practice. Definitely not an EMR. It took two seconds to find the magic formula. Not only was the problem solved, but I gained a deeper understanding of the nature of my dad’s private practice.
Twelve years later, my parents went to the Art Institute on a Sunday in January. When they came home my dad shoveled the drive free of snow so he could make rounds the next day, but the next morning he didn’t wake up. Dr. Bobby Wroten waited in the All Saints doctors’ lounge until I finished my case, then told me my dad had died. I took the last plane that landed that afternoon before O’Hare was closed due to a gigantic snowstorm, and then caught the last cab home. Three days later O’Hare had just reopened, and outside the funeral home across the street from my dad’s office, the plowed snow was piled six feet high on the sides of every street, including down the middle of busy Cermak Avenue; the sidewalks were barely passable, and it was 26 degrees. Once upon a time, an acquaintance had insisted that the number of people who came to a funeral depended on the weather. The line of people who came to bid my dad farewell filled the funeral home and stretched outside more than a block long. The viewing lasted past closing, well into the night.
That was my first experience with my dad’s “family practice” and medicine in the sixties.
From the Achieves: This Last Word was originally published in the September 2017 issue of the Tarrant County Physician and has been edited for clarity. You can read find the full reprint along with the rest of the content from the July/August 2022 publication here.
He was an amazing businessman. His acumen, combined with an ability to take the required risks, helped him to build an automobile repair empire. His smile was infectious. With it, he instilled a fierce sense of loyalty in his employees and business partners. And his words. His Texan twang was musical and fierce. He could cut a deal in seconds with a “Howdy Y’all” and then a “Sign here . . .” That’s how he won the heart of his high school sweetheart. He danced with her from the prom, where he was the King, all the way to the white-washed wedding chapel. They had four children, each one more beloved than the previous, each with that same smile. When he first came to me, I could see what they all loved in him. Despite always being short on time, I would spend the extra few minutes just to laugh at his latest story. I would adjust his blood pressure medication. Somewhere along the way, I added a statin. He did not smoke, and he had no family history. He was doing well, and so that’s why the stroke came so unexpectedly. Four years ago, the conditions changed. The stroke took the entire right side of his body. He couldn’t walk. He couldn’t use his right hand and arm. He was immediately wheelchair-bound. That was not the worst of it, though. The worst was when we found out that he had lost his voice.
The stroke hit his speech centers. He developed an expressive aphasia. He could understand everything that was said, but he could no longer utter a word. The damage to Broca’s area was irreparable. His physicians concurred with this assessment. Perhaps we thought his life was over, or at least the life he had built. His wife’s love for him was stronger than that, though. It was stronger than the assault on his brain and body. She kept him in his business. She kept him in the game. She would take him to physical therapy to strengthen his resolve. She took him to speech therapy and learned his language. She brought back his smile.
She took him to work every day. She was his voice in the meetings. He would smile and grunt, and his empire did not crumble. Physically, he was weak, but as a partnership, she and her husband held strong. I remained amazed by all of this whenever I saw them in clinic. Here was a strong man brought to his knees by a stroke that should have ended him, but instead, he flourished. He flourished because he had a partner that stood by his side always. Even as we did not, she understood his every unintelligible utterance, his body language, and above all else, his smile.
I am given the honor of seeing them periodically in the office. He has had a hospitalization here and there, and she remains his constant companion. She is his advocate. She is his voice. Despite everything we think we know about medical science, she has proven that he is unbreakable.
I often wonder about the intricacies of their relationship. I wonder at his wife’s ability to understand him. Most of all, I marvel at their resilience. Despite overwhelmingly insurmountable odds, they have survived.
Most of all, I marvel at their resilience. Despite overwhelmingly insurmountable odds, they have survived.
There are so many life lessons I have learned from my patients over the years. I want to bring only one of these to all of you. Together, we are stronger. Despite any of our individual weaknesses, we can always give a voice to one another. This becomes especially true in our partnerships and relationships outside of our practices. I am a dinosaur on an island. I am a solo internist. How do I ensure that my voice is heard? I can promise you that the people in Austin and Washington think they know what it is I need and I want. They think they know what we are saying. They think that they can fix medicine. Meanwhile, we think that they are listening to us. We believe that our intelligence and our charisma will carry the day. This is in fact our greatest strength and our greatest weakness. We know we have the answers on how to fix healthcare. I know this to be a fact. My fellow physicians, I have heard all of you loud and clear over the past several months. I have had amazing conversations. I have gained so much insight into my own difficulties in medical practice, and I have come to a better understanding of so many of the difficulties many of you face in your day to day. Some of these discussions have led to even deeper insights . . . But there is the rub. How will we get to action? Action requires us to understand our greatest weakness. We help others all day long, and even though we think we have all of the answers, we are unable to really express them. We too have a form of Broca’s aphasia. I would assert that we need a partnership to make absolutely certain our voice is heard. I believe the partner that binds us all together is the Tarrant County Medical Society, in conjunction with the Texas Medical Association. Many of you have expressed your inability to completely agree with this. We don’t always agree with our partners 100 percent of the time. (Don’t tell my wife this!) Moreover, we need a partner and an advocate that speaks our language and understands us.
Maybe I’m just preaching to the choir. In the end, we will all need to continue to work together, not individually . . . We must come together and make sure that our voice is heard loud and clear . . . They will hear us. Kumbaya. My name is Hujefa Vora, and this is our Last Word.
This article was originally published in the July/August 2022 issue of the Tarrant County Physician. You can read find the full magazine here.
Texas is suffering a healthcare crisis from a lackof practicing physicians. This fact is even graver in rural communities, where the nearest hospital might be a couple of hours away. It is time that we take medical care closer to these vulnerable patients, and that is where mobile healthcare clinics can offer an efficient solution.
As a first-year medical student at the Texas College of Osteopathic medicine, I was fortunate enough to serve with the Pediatric Mobile Clinic at the Health Science Center. To picture this mobile clinic, you must imagine a bus or RV that has been transformed into a fully functional pediatric clinic. It might seem like there would not be much space in the mobile unit, but it is fully equipped to perform many medical services. The unit carries out vaccination drives, full screen wellness check-ups, sports physicals, and much more. It is a small glimpse into the future of medicine.
Looking back at my very first day serving as a student doctor, I did not know the extent of what the pediatric mobile clinic could do. My first patient came in and presented with learning difficulties, café au lait spots, and some vision problems. It was an enormous surprise to find myself examining a possible case of neurofibromatosis, a rare disease that we had covered just a few days prior. I left that day thinking about how this child would not have been able to receive care or be referred to a specialist if the Pediatric Mobile Clinic had not shown up at his school. I felt grateful and fortunate to have been there to serve the children of our Fort Worth community.
It was not until I had a chance to serve in this mobile unit that I realized that this concept was a great solution for Texas’ rural communities. Mobile clinics bring medical services to areas that are hours away from major cities with large medical centers. These clinics are easily adaptable and can be transformed to house many different kinds of practices. They operate much like a regular clinic; patients can look up when the mobile clinic will be near them and then schedule appointments online. Primary care practices can take full advantage of transforming and adapting the mobile units to serve a specific patient population.
For example, mobile clinics can directly help many underserved communities by being closer to patients, which saves time and transportation costs that can often be barriers to seeking treatment. Mobile health clinics do require an initial capital expense for institutions and hospitals. However, they bring in enough revenue to cover their own costs, they draw patients into the sphere of the base clinic or the hospital, and they help keep our community healthier.
I did not expect to feel so strongly about the concept of mobile healthcare clinics when I first set foot onto that crowded bus, but it is impossible not to recognize how efficient it is to have mobile clinics at our major schools and hospital institutions, as well as in rural communities. These mobile clinics should be part of our vision for the future of healthcare. It is time to advocate for more mobile clinics on our Fort Worth roads!