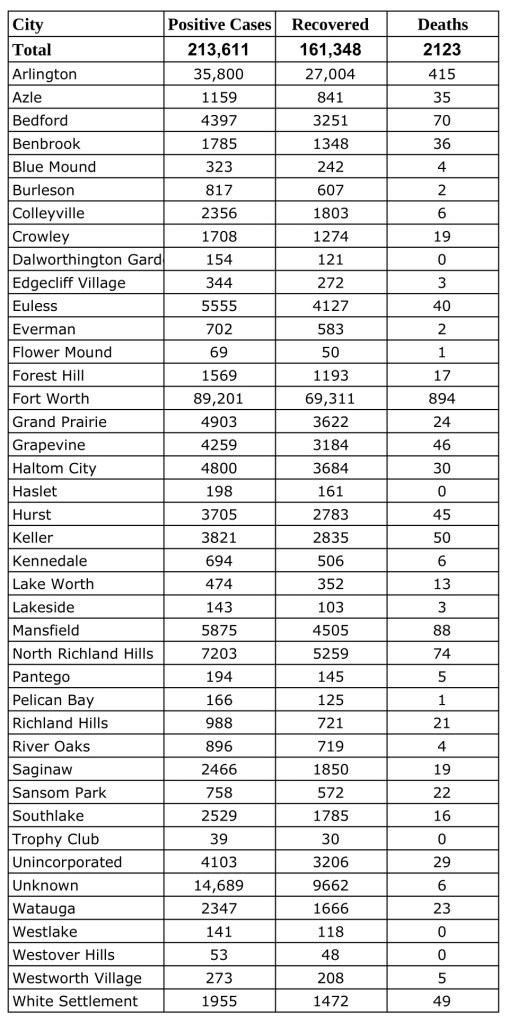
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Thursday, January 28, 2021.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
This piece was originally published in the January/February issue of the Tarrant County Physician. You can read find the full magazine here.
Dr. Angela Self always had an independent spirit. At age 17, fresh out of high school, she left her home in Las Vegas to make a life for herself in New York. As she was growing up, Dr. Self did not dream of becoming a doctor, but she never shied away from an adventure. Looking back, she thinks the decision to pursue Medicine shouldn’t have been such a surprise. When she was 14, Dr. Self volunteered as a candy striper at Southern Nevada Memorial Hospital (now University Hospital), and shortly after she moved to New York, she began working as a dental assistant. “Maybe it was a foreshadowing, but I had never even considered that I would go into Medicine,” says Dr. Self.
The idea to shift directions came suddenly. One day, after assisting with a procedure, Dr. Self began questioning her path. She was filled with a desire to care for patients directly in a capacity where she could serve as their advocate. Medical school came to her as the obvious answer, but she knew it would be a long, winding path. She did not yet have an undergraduate degree so she approached the decision thoughtfully. “Through a process of prayer, and seeking, and volunteering at my ambulance corps, I really felt a strong leading that I was to go to medical school. Once I knew I was going, there was no question in my mind from that moment.” When she felt confident that this was her future, she quickly began making changes to prepare for the long years of study that lay ahead.
Dr. Self realized that she would need a flexible job to support her education, one that would give her freedom to go to classes during the day. She was also hesitant to step away from the clinical interactions she had with patients as a dental assistant. “I thought, it’s going to be eight years before I can do anything,” remembers Dr. Self. “Here I had been working as an oral surgical assistant, a dental assistant. I had been in ORs with an oral surgeon and had been able to do hands-on things.” Because of this, as she began attending classes at a local community college and continued to work full time, Dr. Self also received training as an EMT and a paramedic.
She joined South Orangetown Ambulance Corps in 1987. It was an exciting but hectic time. Dr. Self had three different jobs at that point and picked up extra shifts on the ambulance whenever possible. She worked nights, clocking an average of 60 hours a week while still taking a full load of classes. Despite her long work hours, she was hesitant to slow down. She transferred to Pace University in 1990 and graduated with a BS in Biology in 1992.
At that point, Dr. Self ran into some barriers. She applied to medical school in New York but ended up being waitlisted. Because of her extreme work hours, she had not been able to maintain a 4.0 GPA. Dr. Self was concerned that this would stop her from going to medical school; it was the first time she began to doubt that she had made the right decision. She considered several alternatives, such as pursuing social work, becoming a pharmacist, or even getting an advanced nursing degree.
“Dr. Angela Self is an amazing colleague who I have the pleasure to work closely with on many projects. She is compassionate, honest, hardworking, and has everyone’s best interest at heart. I have the utmost confidence that she will represent Tarrant County Medical Society with dignity, compassion, and will be an overall amazing leader.” – Neerja Bhardwaj, MD
Then, a new opportunity arose. “A friend that went to St. George’s in Grenada suggested that I apply there,” says Dr. Self. She knew it would be a big change—Dr. Self hadn’t planned to leave New York for medical school, much less the U.S. Still, she was intrigued. “I had a couple of friends that I really admired that were going to St. George’s,” she shares. They were very positive about the school, so she decided to apply. She was accepted into the program and began classes in 1994.
Looking back, Dr. Self realizes that she could have applied to other U.S. medical schools, but she has no regrets. Living in Grenada gave her the opportunity to learn hands-on about diseases that are rarely seen in the States, due to Grenada being a developing country. She also gained some wonderful mentors at the school, including Dean of Students Dr. C.V. Rao. “He taught us, he mentored us, he watched out for us, and remains a friend, I think, to everyone who ever went there.”
While in medical school, she was on call for student emergencies. She also continued picking up shifts as a paramedic whenever she was on breaks. It was difficult to work so much while completing her education, but the benefit of financial security coupled with the valuable patient care experience made it worthwhile.
Dr. Self moved back to the U.S. in 1996 to complete her clinical rotations, working between New York and Baltimore. She graduated from medical school in 1998 and began an internship in anesthesiology at the Medical College of Virginia in Richmond. Though anesthesia was appealing, she had a passion to care for geriatric and terminal patients, so she believed her future was in oncology.
At this time, Dr. Self had a big life change—she gave birth to her daughter, Whitney. She took ten months off to care for her young child, until they moved to Texas. At that point, Dr. Self completed her internal medicine residency at St. Paul Hospital in Dallas. It was a difficult time to be going through the intensity of residency. “It was really hard to go every day because I felt I was robbing my daughter of having a mom,” says Dr. Self. She is grateful to her mother for taking care of Whitney, filling the gap when Dr. Self couldn’t be there.
As she completed her residency, Dr. Self fell in love with primary care. She was also ready to focus on her future. “I needed to commit to motherhood and Medicine, and I felt I could do that by doing internal medicine,” says Dr. Self. When she finished the program, she joined a private practice. Dr. Self worked as an internal medicine physician for 15 years. She was employed at three different clinics throughout that time; at one point, she worked for David Pillow, MD, a well-known pillar of the Tarrant County medical community. “Dr. Pillow taught me that patients will tell you what’s wrong if you just listen,” says Dr. Self. He helped her to avoid developing tunnel vision when treating her patients. “His physical exams were amazing. He taught me so many things that you never learn in medical school.”
Dr. Pillow’s guidance along with an extensive background in emergency care made Dr. Self a strong diagnostician. She was quickly able to discover the root of a problem, especially when critical treatment was required. Twice, she was able to get patients immediate care when they came to appointments mid-heart attack, even though their symptoms were irregular. Because she wanted to serve older patients, whenever she joined a new clinic, the Medicare patients were sent her way. “I got the ones with heart failure, liver disease, lung disease, and cancer, and then I got involved with hospice. That fulfilled that longing in me to work with end-stage patients. I did get to do what I wanted after all.”
Still, there was a downside to private practice; it was difficult to manage financially. “Medicare didn’t pay that much, and geriatric patients take a lot more resources, need a lot more time, so you see fewer in a day and reimbursement is lower, but it was what I was passionate about so I did it as long as I could.”
Eventually, Dr. Self made the move to working in administrative medicine. She has been on the other side of care for about five years now; currently, she is working for an accountable care organization. Though she misses taking care of patients, there are many advantages to her current role. “I can advocate for more people in an administrative role than in a primary care practice, where I might have one to two thousand charts, so I can affect one to two thousand lives in practice,” shares Dr. Self. “Now I can affect many more lives.” One of her focuses is improving the patient experience in post-acute settings.
While the change may seem dramatic, Dr. Self has been involved in organized medicine her whole career and has seen the impact of physicians advocating for their profession. She has been a longtime member of TCMS. In the early 2000s, she helped to review cases for the Public Grievance Committee. Dr. Self became more involved during the 2014 Ebola crisis. She was impressed by the way TCMS, TMA, and the AMA worked together to protect patients and physicians, and she knew that was something she wanted to be a part of. “Ever since then, I’ve made attending TCMS’s monthly board meetings part of my job negotiations!”
Dr. Self Is an active member of the TCMS Board of Advisors and the Women in Medicine Committee; she also attends TMA and TCMS meetings whenever possible. “(TCMS board member) Gary Floyd says, ‘Good doctors take care of their patients. Great doctors take care of their patients and their profession,’” says Dr. Self. “Being part of organized medicine is helping to take care of your profession. When doctors go down to Austin and speak with lawmakers in their white coats, it changes the way that we are viewed.”
Her fellow physicians look forward to seeing her in this new role as president. “Dr. Angela Self is an amazing colleague who I have the pleasure to work closely with on many projects. She is compassionate, honest, hardworking, and has everyone’s best interest at heart,” says Neerja Bhardwaj, MD, a palliative care physician practicing in Dallas. “I have the utmost confidence that she will represent Tarrant County Medical Society with dignity, compassion, and will be an overall amazing leader.”
In the next year, Dr. Self hopes to grow physician membership and participation in the Medical Society. She believes in the power of banding together to give doctors a voice for their profession and their patients. She also wants to serve as a resource, particularly for independent physicians who are struggling with the fallout from COVID-19. She thinks providing opportunities to connect with other physicians is an important part of this support. “Talking with other doctors who have experienced the same things helps,” shares Dr. Self. “I’ve been there.” All of this ultimately comes together for one purpose: to serve patients excellently and effectively.
When advising those who are considering going into Medicine, Dr. Self encourages getting as much exposure as possible before taking the leap. “Make sure you have fully answered the ‘why’ for medical school,” says Dr. Self. “Make sure it is something you are passionate about.” Shadow a physician, work as a scribe—whatever it takes to make sure you have found your calling in life. It isn’t an easy path, but it can be incredibly rewarding. “There is nothing else I would rather do.”
When Dr. Self is not working or attending meetings, you might find her volunteering at the Cornerstone Assistance Network. Even though she doesn’t currently practice in a clinic, Dr. Self still enjoys getting to treat patients, especially those who are struggling to access care. In her free time, Dr. Self loves traveling and going to live concerts. Last year she was able to attend the Eric Clapton Guitar Festival. “It was amazing and made me realize that I love the Blues. I didn’t know I loved the genre before that!” A highlight of her trips is always searching for the best lattes in hole-in-the-wall cafés. Dr. Self loves coffee—she even runs a blog to talk about her caffeinated discoveries (you can read some of her stories at coffeebyangela.com).
She enjoys going on these trips (when there isn’t a pandemic!) with friends and family. Dr. Self has the most fun when her daughter can come along, but Whitney is pretty busy these days. She is currently working on completing her undergraduate degree with the goal of applying to medical school in the near future.
We are excited to support Dr. Self as she prepares to lead us as we serve the citizens of Tarrant County and the community of Medicine.
This piece was originally published in the January/February issue of the Tarrant County Physician. You can read find the full magazine here.
Though I vowed not to touch the pandemic as a topic, it seems to be the one thing that’s on my mind. Still crazy after all these months.
I was in Florida when I saw President Trump come on television and announce that we were facing some big changes due to the coronavirus. What I remember most was that his face was white as a sheet and his voice, uncharacteristically, had no dramatic intonation. The serious look on his face and the coming lockdowns scared me much more than the thought of running out of toilet paper. I knew we were headed for a major disaster in this country and it hit me in the gut, hard. I cried easily and often for the next two weeks. I mourned the loss of my country. I knew that many would die, that we would be divided over the handling of the pandemic, and that the pandemic would be highly politicized. I kept changing the channel that March day in 2020. Forgetting Sarah Marshall was needed, and fast. It was an election year and we were already dealing with the polarity of being either a Democrat or a Republican, and now we would be divided over COVID-19 controversy. Let me just say that I have never, ever wanted to get sick from anyone in any public place who was coughing and spewing infectious particles. Masking is about the best idea I’ve ever heard of; I think it’s a great way to decrease disease spread during every cold and flu season, as well as in a pandemic. I once missed Thanksgiving with my family after my sister called and said, “We’re going, but John is sick and he’s running a fever.” I took the next exit off of I-35, turned around, and spent Thanksgiving home alone. It was worth it.
This past January I was speaking with a girlfriend who was getting over a pretty bad upper respiratory infection. She wasn’t sneezing or coughing, but as we talked a little spit droplet flew out of her mouth and into my eye. When that happens, and it does, I just say, “Whatever they’ve got, you’ve got it now.” I do not get that close, or face to face, to this friend anymore. Some people have to spray it when they say it, and COVID-19 is the last thing you want to have sprayed in your face. Looking back over this year I remember a few of my friends had severe upper respiratory infections. Was it COVID-19? Maybe. It seems like years ago that it was okay to cough or sneeze in public, but not now, and it’s just been a little over nine months. Now when a dust particle brings on an unexpected sneeze, the next thing you hear is, “It’s just allergies, I’m not sick!” I agree with stringent infection control measures in public places. I am saddened, however, by businesses closing, millions losing their jobs, nursing homes not allowing any visitors in a safe, distanced way (meaning little accountability and possibly increased neglect), and healthcare professionals using their credentials to further polarize an already confused society.
“Masking is about the best idea I’ve ever heard of; I think it’s a great way to decrease disease spread during every cold and flu season, as well as in a pandemic.”
So what do we do? How do we move forward? I have a friend who lost his wife to COVID-19 months ago (she was an ER nurse in New Jersey), and I have another good friend who just recovered from COVID-19 pneumonia. This virus is still a public threat. People are still dying. Treatments are helping many, but like the flu and other diseases, there is not a cure. A vaccine will not be 100 percent preventive. It’s the best we’ll be able to do, but it won’t be 100 percent. Do we allow our economy to collapse or do we get back to work in a safe and smart way? It’s easy for those of us who can go to work to say, “Stay home,” as we are able to provide for our families. During this pandemic, I went to a certain coffee shop every day and sat at a table outside with my cousin (it was the only contact that the both of us had with another person during the early days of the pandemic). We would see other coffee friends pull up and have their orders delivered to their car. We watched the mask requirement come in and we complied; we still do. The thing that we mostly did was sit there every morning and act normal while supporting a struggling local business. We were socializing over coffee in a safe manner. If I had to cough (allergies) I would get up and walk around the side of the building. In the spring, if the group ever grew to over the allowed number, someone would leave and let another sit and visit. Our coffee shop owners had to lay off twenty employees and close their shop in Southlake. One of the negative consequences, besides death from illness and job loss, is depression that has been made worse due to social isolation. Though many of us feel we can safely get our groceries, have our coffee, and take care of business, as long as the protective measures are being used, there are still many who are very afraid. That fear has likely served the most vulnerable well, as they’ve had limited exposure to COVID-19, but it has cost others their lives due to depression and suicide. It has cost some child abuse victims their lives, with school being a safe place where they could escape the abuse for at least a few hours. I am grateful that Texas has allowed businesses to reopen and let our citizens get back to work and their kids back to school. This pandemic is not over yet, but hopefully, much of the devastation is behind us as we learn more about this virus and how to best treat it.
The way I would like to see us move forward is with safety protocols and measures in place, while returning to our livelihoods with moms and dads able to pay the mortgage, keep the lights on, and feed their kids. Talk about “social determinants of health”; can we even measure the food insecurity that’s out there when we’ve taken a meal away from a kid who might not get any meals at home? Let’s move ahead with disease prevention. How many mammograms and colonoscopies were not done this year, leaving cancer undiagnosed and untreated? I’ve seen some “quality” scores and there are many “gaps” that weren’t closed in 2020. The thing about open gaps is that you just don’t know which gap closures would’ve caught a disease process in its early stages.
I wanted to start off the year with an article about avoidable hospitalizations from UTIs gone wild or how medical directors are people too, but instead, I have broken my own rule about avoiding controversy. If you’re a little confused on where I stand on COVID-19, here are my thoughts: 1) respect your fellow man by wearing a mask and keeping a safe distance; 2) consider if you might be putting a high risk person at increased risk (self-quarantine if you’ve been exposed); 3) be kind to each other as many are struggling with the loss of friends, family, personal health, or their job; 4) exercise your rights and freedoms in a safe manner; 5) the virus is very real and very deadly (to some even previously healthy people); and 6) take the vaccine if you get the opportunity—it’s the best we can do to turn the tide on this pandemic. Blessings, and I look forward to an America without COVID-19.
This piece was originally published in the January/February issue of the Tarrant County Physician. You can read find the full magazine here.
How we communicate with patients has changed a lot over the years. Millennia ago, having little to offer by way of effective medical intervention, healers relied on therapeutic relationships. What healing occurred was largely due to the relationship itself. Priests, shamans, witch doctors, medicine men, and the like were important threads in the social fabric of their communities. Caring for both spiritual and physical needs, they functioned in roles that we recognize today as clergy and physician.
In the second millennia, and especially after the Enlightenment, these twin traditions of healing began to unwind. As scientific knowledge in general, and medical knowledge in particular, became increasingly robust, the role of the physical healer became distinct from that of the spiritual healer.
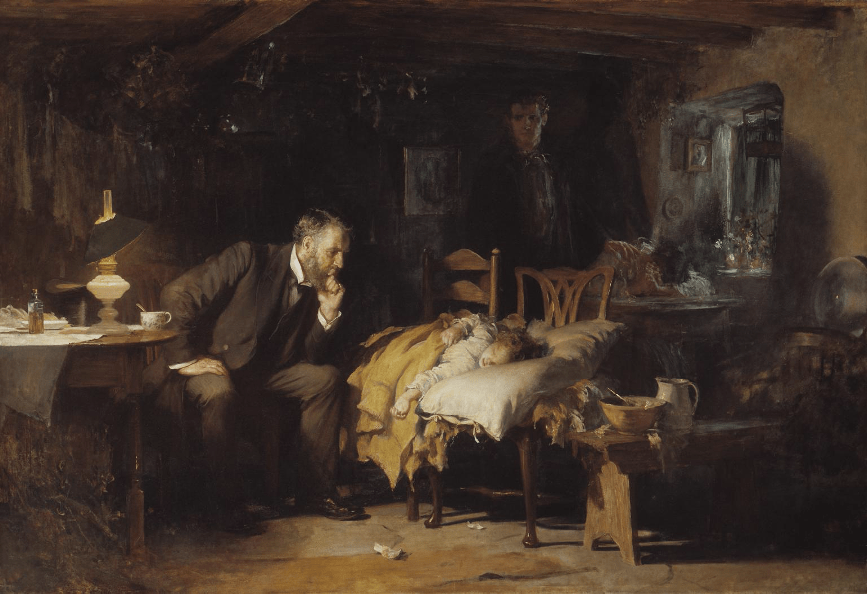
“The Doctor” by Luke Fildes (1891)
While the physician’s library of remedial options increased, it remained limited until the 20th century. Instead, relationships and trust continued to be the bedrock of the therapeutic encounter. “Being there”—itself a form of communication—was as important as the intervention. A beautiful illustration of this is Luke Fildes’ 1891 painting, “The Doctor,” depicting a physician sitting at the bedside of an ill child, the concerned parents in the peripheral shadows. The physician appears to be doing nothing but sitting there looking concerned, but that’s the point. “Being there” is doing something and speaks volumes to the parents who simply want to know that someone cares enough to exercise everything in their power, limited as it may be, to effect a cure.
With the Information Age came a breakneck pace of scientific innovation. In 1900 the definitive textbook of internal medicine was Osler’s The Principles and Practice of Medicine. It had one author: Sir William Osler. But by the 1950s the expansion of medical knowledge required that the definitive textbook—the first edition of Harrison’s Principles of Internal Medicine (1951)—had 53 authors.1 The era of specialization had arrived.
Along with it came a gradual dissolution of the longitudinal and relational nature of patient-physician encounters. Increased specialization meant we could do more to effect a cure, but the more we could do, the more distant physicians became from their patients.
I trace the origin of this—because it works as a metaphor on multiple levels—to French physician René Laennec’s invention of the stethoscope in 1816. One day he observed schoolchildren scratching the end of a hollow stick to hear the amplified sound at the other end. He applied this acoustic principle to solve a problem he was facing regarding the examination of a patient. As Laennec put it, he had been
“consulted by a young woman laboring under general symptoms of diseased heart, and in whose case percussion and the application of the hand were of little avail on account of the great degree of fatness”2
Given her age (young) and gender (female), direct auscultation was not an acceptable option anyway, so recalling the children’s game he rolled up a piece of paper and listened to her heart. The stethoscope was born, a technological innovation had occurred, and the physician took the first step away from the patient.
As medical specialization grew so did that distance. Now we don’t even need to be on the same continent. Physicians, as masters of applied science, assumed the role of the expert who diagnosed a condition and recommended a course of action to a patient. The patient then largely deferred to the physician’s judgment and expertise, reinforcing the benevolent paternalism that had been implicit in patient-physician encounters for generations, only now it had a name.
Popular culture was replete with examples of benevolent paternalism, perhaps best embodied by actor Robert Young who played the lead role in both Father Knows Best (1954-1960) and Marcus Welby, MD (1969-1976). His character was similar in both series. He was the trusted expert, and those in his charge did what he told them to do.
Or did they? Patients actually doing what they are advised to do is every bit as important as the advice itself. We came to realize what the priests, shamans, witch doctors, and medicine men knew millennia ago: personal relationships built on a foundation of trust and effective communication are important. If the primary endpoint is healing the patient, we must be able to communicate the pathway that gets them there, which means we must understand and help them navigate around the roadblocks they will encounter along the way. These could be social, cultural, linguistic, ethnic, racial, intellectual, and/or economic, to name a few. Dr. Welby may have arrived at the correct diagnosis and recommended an appropriate evidence-based course of treatment, but what good is that if the patient won’t—or can’t—follow through with it?
Twenty-five years ago, the correlation between effective physician-patient communication and improved health outcomes was already obvious.3 The body of evidence has only grown, demonstrating that providers who are good communicators obtain more complete information, arrive at more accurate diagnoses, and facilitate more appropriate counseling, all of which increase the likelihood that patients will adhere to the plan.4 And if that doesn’t get our attention, good communication has also been shown to reduce the likelihood of a lawsuit.5
Locally, the importance of effective communication has been underscored by the creation of a dean level position at the UNTHSC-TCU School of Medicine, the highest position ever dedicated to this important aspect of patient health at an American medical school. We should be proud that this occurred in our county, but it’s just a beginning. There are many layers to this onion, and it will take more than an emphasis at a medical school to peel it. For those of us who are already in practice—many for decades—we are learning to communicate in new ways. A year ago, telemedicine consults were not on my radar at all. Now I have several every day. These newer forms of communication and patient interaction, coupled with a better understanding of what effective communication actually is, introduce additional challenges to the patient-provider relationship.
Recognizing the timeliness and rapid evolution of this topic, Healthcare in a Civil Society, the annual CME hosted by TCMS’s Ethics Consortium, will dedicate its 2021 symposium to effective patient communication. As the era of shared decision-making has moved forward, so has our need to communicate with our patients in meaningful and relevant ways. This program will explore how communication between providers and their patients has changed, and the ethical implications this change has had in a variety of areas.
AMA President, Dr. Sue Bailey, will keynote this Zoom event which has been generously supported by UNTHSC and the Cook Children’s Medical Center Foundation. The Hon. Pete Geren will moderate an expert panel who will address topics such as:
Shared Decision-Making – How can we know that a medical decision is truly “shared” and the consent obtained truly “informed”?
Truth-Telling and Apology – How do we communicate with patients about difficult topics, especially when something goes wrong, or we make a mistake that results in patient harm?
High-Stress Conversations – How does our communication with patients change when providers are in a high-stress situation, and how can providers self-regulate and/or de-escalate a contentious conversation?
Patient Communication (in general) – What can we all do that will engage patients and foster relationships in which information can be shared in a meaningful way?
The event includes a breakout session to allow participants to explore the topic more deeply in small groups.
Effective patient communication has come a long way in recent years, but we have a long way still to go. All are welcome to join us for this informative and interactive session. You can view a flyer with registration information here.
Sir William Osler (1849-1919)
References 1The exponential growth of medical knowledge can be illustrated by tracking the number of authors for the definitive textbooks. As noted, by 1951 Harrison’s Principle of Internal Medicine had 53 authors. By the time I was in medical school it had 273 authors. Today it has over 600. Plot it on a curve. It’s exponential.
2From René Laennec’s De l’Auscultation Médiate, quoted in Laënnec and the Stethoscope. JAMA. 2019;322(5):472. doi:10.1001/jama.2018.15451
Stewart MA. Effective Physician-patient Communication and Health Outcomes: A Review. Canadian Medical Association Journal. 1995; 152(9):1423-1433.
3Effective patient–physician communication. Committee Opinion No. 587. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014;123:389–93.
4Virshup BB, Oppenberg AA, Coleman MM. Strategic Risk Management: Reducing Malpractice Claims Through More Effective Patient-Doctor Communication. American Journal of Medical Quality. 1999;14(4):153-159.
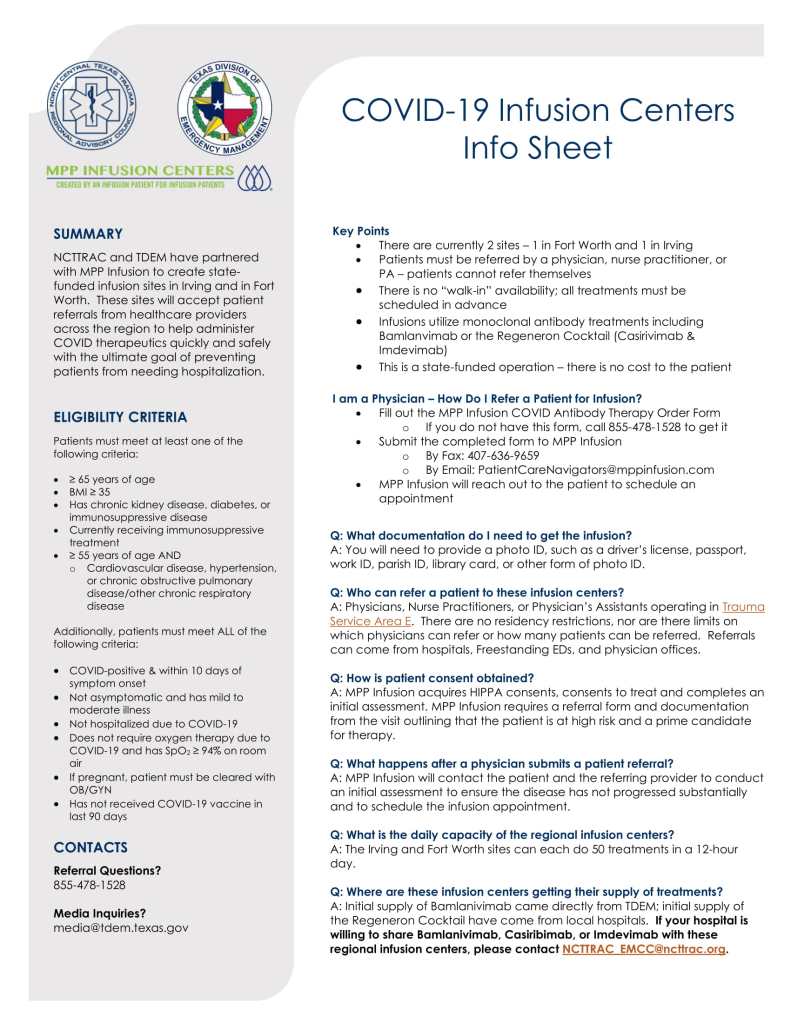
Below is the current information about Tarrant County’s COVID-19 Infusion Centers. You can find a more readable version of the information sheet with functioning links here.
You can find the Infusion Centers Referral Form here.
Key points to remember:
There are currently two (2) Infusion Center sites in Tarrant County
Patients must be referred by a physician, an NP, or a PA
Walk-in appointments are not available
There is not cost to the patient for treatment
If you have referral questions, call (855) 478-1528.
Join us as we install Angela Self, MD, as TCMS’s 2021 president. The ceremony will take place over Zoom at our January Board of Advisors meeting, which will be held Wednesday, January 27, 2021, at noon.
If you would like to participate, email Melody Briggs at mbriggs@tcms.org.
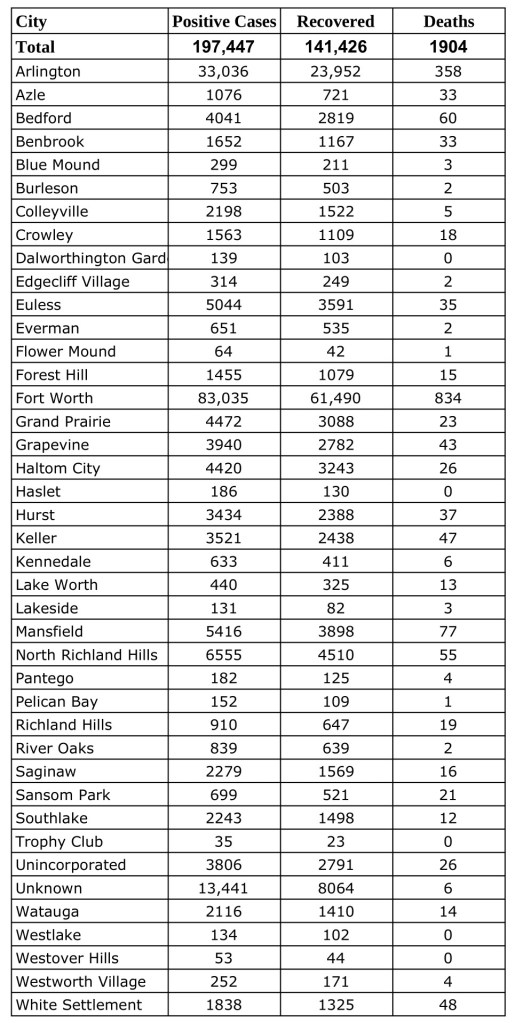
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Tuesday, January 19, 2021.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
The challenges of 2020 changed us, but they did not stop us. A look at how PATC adapted during unprecedented times.
By Kathryn Narumiya, PATC Program Director
Happy New Year!
One year ago, few would have thought that in just weeks, our places of business, worship, and pleasure would be severely limited or closed. Fewer still could have predicted the profound effect this would have on patient access to medical care.
Project Access Tarrant County was similarly affected. Sometimes we wondered how the program would continue. But, true to PATC tradition, we evaluated, collaborated, and devised a plan that fits our current reality.
Instead of attending in-person intake sessions with PATC staff, patients now complete the process virtually. Instead of delivering documents to the office, patients fax or mail them. And while some of our patients have had to be creative in how they access the necessary technology (who hasn’t?), every one of them has been able to make it work.
Reflecting on 2020, we are amazed at how much we were able to accomplish given the shutdowns and hospital limitations. PATC coordinated 382 medical appointments for 105 patients, including 20 surgeries and other hospital procedures during a period when access for even paying patients was severely limited.
We are always grateful for our volunteers and partners, but this year, we are especially thankful for our generous volunteers who continued to see patients and provide charity care during a time of uncertainty.
As I write this, hospitals are reaching capacity (again) and are postponing and canceling surgeries and procedures. As a result, PATC has several patients whose cases are on hold indefinitely. But this time, we know how to proceed. We have a plan and we will continue to take each day and each moment one step at a time until we reach the other side.
Tune in tonight at 7:00pm on the North Texas Medical Society Coalition Facebook Page for another great live discussion with your community physicians. This week, Dr. Mark Casanova (Dallas County Medical Society) and Dr. Bryan Johnson (Collin-Fannin County Medical Society) will host Dr. Gregorio Gomez from the University of Houston College of Medicine for a conversation on the science behind the COVID-19 vaccines.