by Stuart Pickell, MD, MDiv, FACP, FAAP
This piece was originally published in the January/February issue of the Tarrant County Physician. You can read find the full magazine here.
How we communicate with patients has changed a lot over the years. Millennia ago, having little to offer by way of effective medical intervention, healers relied on therapeutic relationships. What healing occurred was largely due to the relationship itself. Priests, shamans, witch doctors, medicine men, and the like were important threads in the social fabric of their communities. Caring for both spiritual and physical needs, they functioned in roles that we recognize today as clergy and physician.
In the second millennia, and especially after the Enlightenment, these twin traditions of healing began to unwind. As scientific knowledge in general, and medical knowledge in particular, became increasingly robust, the role of the physical healer became distinct from that of the spiritual healer.
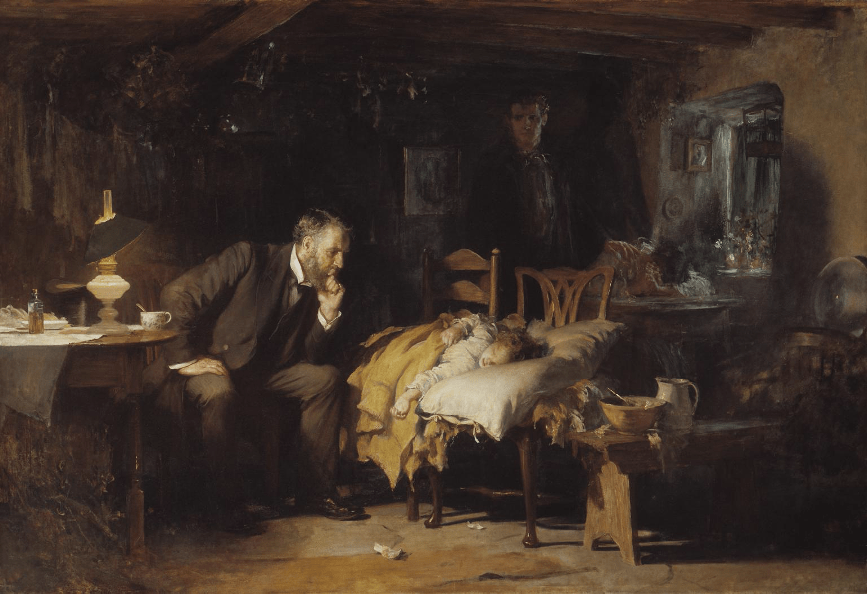
While the physician’s library of remedial options increased, it remained limited until the 20th century. Instead, relationships and trust continued to be the bedrock of the therapeutic encounter. “Being there”—itself a form of communication—was as important as the intervention. A beautiful illustration of this is Luke Fildes’ 1891 painting, “The Doctor,” depicting a physician sitting at the bedside of an ill child, the concerned parents in the peripheral shadows. The physician appears to be doing nothing but sitting there looking concerned, but that’s the point. “Being there” is doing something and speaks volumes to the parents who simply want to know that someone cares enough to exercise everything in their power, limited as it may be, to effect a cure.
With the Information Age came a breakneck pace of scientific innovation. In 1900 the definitive textbook of internal medicine was Osler’s The Principles and Practice of Medicine. It had one author: Sir William Osler. But by the 1950s the expansion of medical knowledge required that the definitive textbook—the first edition of Harrison’s Principles of Internal Medicine (1951)—had 53 authors.1 The era of specialization had arrived.
Along with it came a gradual dissolution of the longitudinal and relational nature of patient-physician encounters. Increased specialization meant we could do more to effect a cure, but the more we could do, the more distant physicians became from their patients.
I trace the origin of this—because it works as a metaphor on multiple levels—to French physician René Laennec’s invention of the stethoscope in 1816. One day he observed schoolchildren scratching the end of a hollow stick to hear the amplified sound at the other end. He applied this acoustic principle to solve a problem he was facing regarding the examination of a patient. As Laennec put it, he had been
“consulted by a young woman laboring under general symptoms of diseased heart, and in whose case percussion and the application of the hand were of little avail on account of the great degree of fatness”2
Given her age (young) and gender (female), direct auscultation was not an acceptable option anyway, so recalling the children’s game he rolled up a piece of paper and listened to her heart. The stethoscope was born, a technological innovation had occurred, and the physician took the first step away from the patient.
As medical specialization grew so did that distance. Now we don’t even need to be on the same continent. Physicians, as masters of applied science, assumed the role of the expert who diagnosed a condition and recommended a course of action to a patient. The patient then largely deferred to the physician’s judgment and expertise, reinforcing the benevolent paternalism that had been implicit in patient-physician encounters for generations, only now it had a name.
Popular culture was replete with examples of benevolent paternalism, perhaps best embodied by actor Robert Young who played the lead role in both Father Knows Best (1954-1960) and Marcus Welby, MD (1969-1976). His character was similar in both series. He was the trusted expert, and those in his charge did what he told them to do.
Or did they? Patients actually doing what they are advised to do is every bit as important as the advice itself. We came to realize what the priests, shamans, witch doctors, and medicine men knew millennia ago: personal relationships built on a foundation of trust and effective communication are important. If the primary endpoint is healing the patient, we must be able to communicate the pathway that gets them there, which means we must understand and help them navigate around the roadblocks they will encounter along the way. These could be social, cultural, linguistic, ethnic, racial, intellectual, and/or economic, to name a few. Dr. Welby may have arrived at the correct diagnosis and recommended an appropriate evidence-based course of treatment, but what good is that if the patient won’t—or can’t—follow through with it?
Twenty-five years ago, the correlation between effective physician-patient communication and improved health outcomes was already obvious.3 The body of evidence has only grown, demonstrating that providers who are good communicators obtain more complete information, arrive at more accurate diagnoses, and facilitate more appropriate counseling, all of which increase the likelihood that patients will adhere to the plan.4 And if that doesn’t get our attention, good communication has also been shown to reduce the likelihood of a lawsuit.5
Locally, the importance of effective communication has been underscored by the creation of a dean level position at the UNTHSC-TCU School of Medicine, the highest position ever dedicated to this important aspect of patient health at an American medical school. We should be proud that this occurred in our county, but it’s just a beginning. There are many layers to this onion, and it will take more than an emphasis at a medical school to peel it. For those of us who are already in practice—many for decades—we are learning to communicate in new ways. A year ago, telemedicine consults were not on my radar at all. Now I have several every day. These newer forms of communication and patient interaction, coupled with a better understanding of what effective communication actually is, introduce additional challenges to the patient-provider relationship.
Recognizing the timeliness and rapid evolution of this topic, Healthcare in a Civil Society, the annual CME hosted by TCMS’s Ethics Consortium, will dedicate its 2021 symposium to effective patient communication. As the era of shared decision-making has moved forward, so has our need to communicate with our patients in meaningful and relevant ways. This program will explore how communication between providers and their patients has changed, and the ethical implications this change has had in a variety of areas.
AMA President, Dr. Sue Bailey, will keynote this Zoom event which has been generously supported by UNTHSC and the Cook Children’s Medical Center Foundation. The Hon. Pete Geren will moderate an expert panel who will address topics such as:
- Shared Decision-Making – How can we know that a medical decision is truly “shared” and the consent obtained truly “informed”?
- Truth-Telling and Apology – How do we communicate with patients about difficult topics, especially when something goes wrong, or we make a mistake that results in patient harm?
- High-Stress Conversations – How does our communication with patients change when providers are in a high-stress situation, and how can providers self-regulate and/or de-escalate a contentious conversation?
- Patient Communication (in general) – What can we all do that will engage patients and foster relationships in which information can be shared in a meaningful way?
The event includes a breakout session to allow participants to explore the topic more deeply in small groups.
Effective patient communication has come a long way in recent years, but we have a long way still to go. All are welcome to join us for this informative and interactive session. You can view a flyer with registration information here.

References
1The exponential growth of medical knowledge can be illustrated by tracking the number of authors for the definitive textbooks. As noted, by 1951 Harrison’s Principle of Internal Medicine had 53 authors. By the time I was in medical school it had 273 authors. Today it has over 600. Plot it on a curve. It’s exponential.
2From René Laennec’s De l’Auscultation Médiate, quoted in Laënnec and the Stethoscope. JAMA. 2019;322(5):472. doi:10.1001/jama.2018.15451
Stewart MA. Effective Physician-patient Communication and Health Outcomes: A Review. Canadian Medical Association Journal. 1995; 152(9):1423-1433.
3Effective patient–physician communication. Committee Opinion No. 587. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014;123:389–93.
4Virshup BB, Oppenberg AA, Coleman MM. Strategic Risk Management: Reducing Malpractice Claims Through More Effective Patient-Doctor Communication. American Journal of Medical Quality. 1999;14(4):153-159.
