Rule ignores statutory text and congressional intent, shrinks access to care for patients
The Texas Medical Association (TMA) filed a lawsuit in federal district court in Tyler, Texas, after the Biden administration failed to follow clear direction from Congress about how to implement the dispute resolution process set forth in the No SurprisesAct, legislation that was passed in 2020 to protect patients from surprise medical bills.
“TMA supports the patient protection intent of the No Surprises Act,” TMA President E. Linda Villarreal, MD, said. “However, TMA’s lawsuit challenges one component of the administration’s rule that ignores congressional intent and unfairly gives health plans the upper hand in establishing payment rates when a patient receives care from an out-of-network physician, oftentimes in an emergency.”
Congress intended to create a fair and unbiased process to resolve billing disputes between health insurance companies and physicians by ensuring that all relevant factors must be considered, with each given the weight deemed appropriate by the arbitrator. In contrast, the administration’s short-sighted approach will make it harder for patients to access care by driving down reimbursement rates and encouraging insurance companies to continue narrowing their networks. It will be difficult for small physician groups to keep caring for patients.
“The lawsuit filed yesterday ensures that the protections for patients against balance bills will go into effect on Jan. 1, 2022, while seeking to stop the imminent harm to physicians and hospitals created by an unfair arbitration process,” Dr. Villarreal said.
The recently released rule rewrites the statute by requiring the arbitrator in the independent dispute resolution process to presume that the qualifying payment amount (QPA), set by health insurance companies for patient cost-sharing purposes, is “the appropriate out-of-network rate.” This creates a bias that prioritizes offers closest to the QPA, rather than allowing arbitrators to exercise their discretion to weigh all relevant factors and select the reimbursement rate that most accurately reflects fair market reimbursement and individual circumstances.
The TMA lawsuit asks the court to strike this section of the rule and instead restore the fair, balanced dispute resolution process that Congress created. The lawsuit also alleges a violation of the Administrative Procedure Act, which requires a formal notice and comment period in advance of finalizing such a rule. The agencies failed to solicit and incorporate comments from stakeholders for this crucial aspect of the law.
“We wholeheartedly agree with U.S. Reps. Richard Neal’s (D-Mass.) and Kevin Brady’s (R-Texas) concern that the rule tips the scale in favor of insurance companies and will leave patients vulnerable,” Dr. Villarreal said. Representative Neal is chair of the U.S. House Ways and Means Committee, and Representative Brady is the past chair of the committee and currently ranking Republican member.
“We are disappointed the Biden administration ignored congressional intent and essentially set up the arbitration system to operate like a casino, with health insurers playing the role of the house,” Dr. Villarreal said. “Everyone knows the house always wins. With the current rule, patients, physicians, and our country lose.”
TMA is the largest state medical society in the nation, representing more than 55,000 physician and medical student members. It is located in Austin and has 110 component county medical societies around the state. TMA’s key objective since 1853 is to improve the health of all Texans.
This article was originally published in the July/August issue of the Tarrant County Physician. You can read find the full magazine here.
I remember working as a medic in New York and New Jersey and loving what I did all day, every day (and many times all night). When I got “the call” to go to med school, I knew that it would be years before I could do anything clinical—at least eight years. My first procedure was at 14 years old at Southern Nevada Memorial Hospital (now University Hospital), when a surgeon let me round with him on a patient and told me to pull the tube straight back. I pulled out a chest tube at 14. Where do you go from there? Well, the day I went back to taking food trays to rooms and getting the nurse when a patient needed their bedpan to be emptied. After high school, I started taking dental x-rays, and I took great x-rays without even using the rings and film holders. I spent those moments in the darkroom praying and soaking in the blessing of the esteemed opportunity that I had been given as an almost dental assistant. Those x-ray skills thrust me into a career in dental and then oral surgical assisting.
When life brought me back to my home state of Texas, I got my first job as an oral surgical assistant. Dr. Robert Thomas Perry hired me after looking at my résumé, which was handwritten on a 11-by-14-inch sheet of legal paper. Full disclosure, when he asked for my résumé, I did not know what that meant; he explained that it was a list of my experience. I was just about 21 years old by then, so he was an early inspiration for me. We would drive to remote sites to perform oral surgeries and I would read board review material to him for hours and hours as we drove from College Station to Corsicana and Huntsville. I learned so much about oral surgery from these hours of drives, which always included a stop for Blue Bell ice cream.
Dr. Perry and his wife, a CRNA, were very well liked in the community, though he struggled to establish great referral patterns from the general dentists. While he was away doing his oral surgery training, two other oral surgeons, Garrett and Gray, had set up practice. Their winning personalities and ability to network between Bryan and College Station proved to be a barrier to Dr. Perry getting much business in this good ole boy country. Dr. McElroy did send us patients. Dr. McElroy is known to have left Thanksgiving dinner for an emergency; he even showed up at his office to meet a patient with a severe toothache one Christmas Day. That patient was one of my relatives (I got him on multiple holidays). Dr. Perry had me credentialed at both local hospitals and one in another town. At St. Joe’s in Bryan, I went through a week-long orientation in the OR, watching various cases so that I could assist Dr. Perry there—I knew all of the instruments he used and when he used them. I didn’t just see oral surgeries; I had a front-row seat for everything that was happening in the OR that week. I remember watching a vag hyst (in horror) and then a breast biopsy where they had to go ahead with a mastectomy right then, after the frozen section came back positive. I was a high school graduate dental assistant, and I was in the OR.
You think it’s difficult to get someone to take a statin? Try telling them you’re going to put a tube down their throat.
I first started assisting Dr. Perry in the OR when he performed orthognathic surgery that included down-fracturing a maxilla. I was so happy and fulfilled in my work. I had arrived. When the local hospitals stopped using CRNAs in the mid 80s, Dr. Perry had to move his family back to Ohio, where he had trained. Sue, his wife, was actually the breadwinner. Dr. Perry once had a farmer pay him with a side of beef (tractor accident). Another elderly woman paid him by making fabric holders for his surgical instruments. He was not the only oral surgeon that I worked for who depended on the income of their spouse to stay afloat. After crying every day for two weeks over having to leave Dr. Perry due to the imminent practice closure, I moved back to New York, where I had lived right after high school. I went to work for another oral surgeon there and I also joined my volunteer ambulance corps.
I was a trainee at the South Orangetown Ambulance Corps when I took my EMT course and then immediately followed with my medic course, which I studied at White Plains Hospital. I worked in Rockland County with my ambulance corps and in Westchester County as part of my medic class. I remember being in Yonkers, where the medics put on bulletproof vests at the beginning of their shift. I drove around White Plains looking for an address where there was a patient with a GI bleed. The police kept telling me to step it up (the patient was bleeding out from varices). Basic Life Support (BLS) transported the patient before I arrived as I was not familiar with White Plains, having lived in Rockland County and only commuting to Westchester. I remember once, when responding to a cardiac arrest, we found upon our arrival that the husband had coded, too. I had to decide which code we would care for, and which one would have to wait for the second unit to arrive.
One time I regretted having taken this career path—it was in the moments before arriving on-scene at an accident involving a train. Thank God for my partner, who also worked for NYC EMS at the time. He was a calm and reassuring voice as we worked with the PD to locate the body parts. This was important, because when daylight came there would be parents driving kids to school and the carnage would be seen in the light of day. There was the time that I dropped my partner at a call with the volunteers (we worked as a pair from a fly car, which is used to carry equipment, and would split up as needed). I arrived at a scene where the wife called about her husband, who was unresponsive. I had to speak to the wife in a calm, reassuring way as I dragged her husband by the feet from the foot of the stairs to the middle of the living room floor where I would intubate, put on the monitor, start an IV and work the code until another BLS unit arrived to transport him to Nyack Hospital. An awake intubation on someone in distress from severe congestive heart failure is an exercise in coaching a patient. You think it’s difficult to get someone to take a statin? Try telling them you’re going to put a tube down their throat.
I knew I wanted to go to med school, but it wasn’t to be in New York, and I didn’t apply anywhere else. While working in White Plains I met fellow medics George Kiss and John Brebbia. They were both students at Saint George’s University School of Medicine. I also knew Dr. Stuart Rasch, an ER doc at Nyack who was an SGU grad. I applied. I got in. I went. I continued to work as a medic per diem during my breaks from school. I worked for several companies at one time—Mamaroneck, Portchester Rye, and Larchmont, which were volunteer agencies with paid medics, and Rockland Paramedic Services and Clifton-Passaic MICU in Passaic, New Jersey. The relationships that I made still endure. The experiences that I had continue to keep the paramedic in me alive. I miss days when I would arrive at the home of an elderly person having an MI or pull up on the scene of an MCI (mass casualty incident). The other day I was talking to a close friend on the phone, and he mentioned in passing that his dad was short of breath. The last time someone mentioned that in passing (in the pulpit at a church), they ended up in the cath lab getting stents the following day. This time it was a friend, and I knew his dad. I calmly asked, “Do your parents mind if I come over?” Though it was late at night, they agreed. I got dressed and went over and did a medic questionnaire and exam which led to an ER visit and hospital stay. Though the family is thankful that I was there, I am even more thankful, because they allowed me the opportunity to remember life when I would wake up and be excited to go to work every day, all day (and many times all night).
Watch below to hear TCMS President Angela Self, MD, explain how the monoclonal antibody treatment, which was recently taken for Fort Worth Mayor Mattie Parker, is an effective tool for COVID-19 treatment.
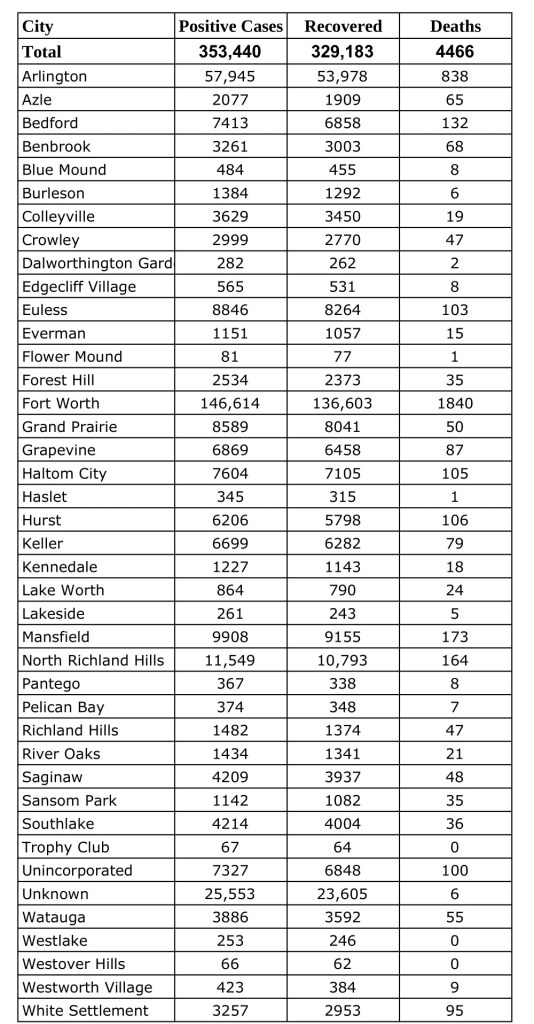
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County updated Monday, October 11, 2021.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
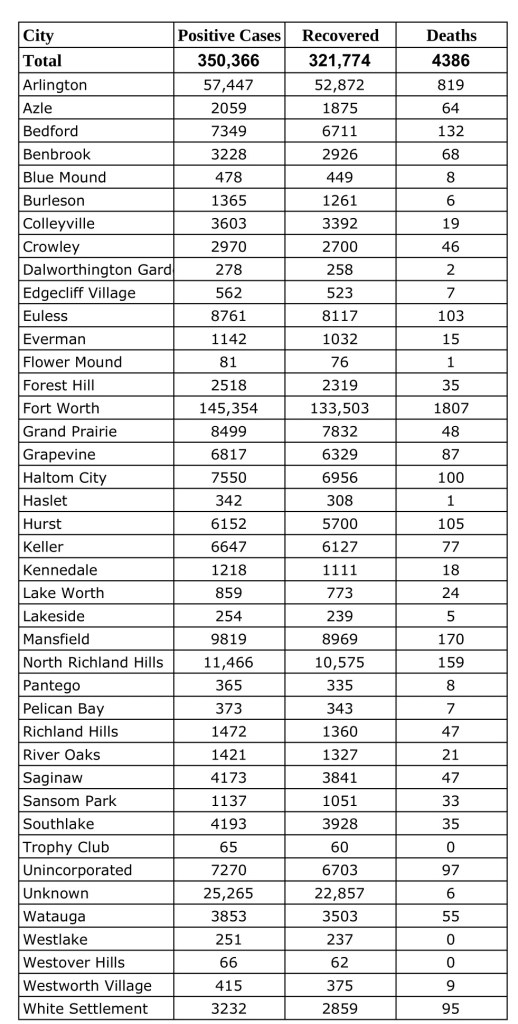
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Wednesday, October 6, 2021.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
Imposter syndrome and how the little monster brings us down.
by Ashley Brodrick, OMS-III
This article was originally published in the July/August issue of the Tarrant County Physician. You can read find the full magazine here.
“Am I really cut out for this?” A question most medical students have asked themselves time and time again. Imposter syndrome is this little monster in the back of our minds that tells us we are inadequate; it grows every week, with every test, and with every medical encounter. It tells us we are destined to fail. It tells us we are never going to make it, we are never going to learn, and we are never going to be good doctors. This little monster puts doubts into our minds about our ability to be successful physicians. If you are lucky enough never to have been visited by this little monster, I applaud you.
Medical school is this arduous four-year journey that tests us mentally, physically, emotionally, and sometimes even brings us to our breaking point. Why is medical training so taxing on our emotions, leaving us feeling empty, drained, and questioning if we are made for this career? Medical school is competitive by nature, with a national acceptance rate of 43 percent. This means you must be the “best of the best,” graduating with extraordinarily high GPAs, and performing well on the MCAT. Don’t get me wrong, being a doctor is no easy task. You are responsible for another person’s life, something that I consider to be a tremendous honor. However, at what point do we start to take a step back and reconsider this competitive atmosphere that we have fostered for so long and look at applicants on a holistic level and not just a statistic on a sheet of paper. I can tell you I would rather have a doctor that understands my concerns and listens to me than one who scored in the 99th percentile on their standardized exams but never questions their diagnosis. I would rather have a doctor that IS questioning their diagnostic and treatment decisions for me—not because they don’t know the proper protocols, but because they care about getting my treatment right for me as an individual. M
I am no stranger to imposter syndrome; however, this little monster did not visit me until my second year. My first year of medical school was the year I thrived, leading me to believe that maybe I could make it through without letting that little monster get the best of me. My grades were above average, I was making friends, and I was becoming more confident in my ability to talk to patients (even if it was standardized and following a script). The real challenge for me came during my second year, when my self-doubt started setting in. I was having difficulty connecting the dots and putting everything together. My classmates seemed to be following the right path, understanding how the different diseases connect across organ systems, whereas I felt like I was stumbling every step of the way. Each block presented a new challenge and fed that little monster even more. While I could understand the information and explain it flawlessly to my friends, it was just not coming together on the tests. This inability to perform well on exams did a number on my mental health. You don’t realize how deep into a hole you are until you turn around and realize you can no longer see any light, making it impossible to escape. Each day I would wake up with my heart racing, but you know what I did? I told myself this was normal; this is what medical school is supposed to be like. Stressful, hard, and exhausting, it takes everything out of you along the way, while proving to everyone that you are the “best of the best,” having the highest level of education, being in the top 0.29 percent of the population. The one thing I did not tell myself was that medical school did not have to be this way.
Medical school puts you in a bubble, one that is hard to escape. You are surrounded by medicine 24/7, and during my first two years I found it difficult to talk about anything other than medicine when I was with my friends and family. Every time I went home it was always, “How is school going? Any recent tests? What are you learning now? Making good grades still?” It was never, “How are you handling everything? Is there anything you need help with?” I knew they were trying to show an interest in my education, and genuinely wanted to know what I was learning, but I did not have the energy to go into detail. So, I found myself falling into the same routine of saying, “School is going well, just the same every day. I spend 10 hours in the library and when I get home I take Sadie on a walk, then sit on my couch and watch TV until I do it all over again.” This wasn’t always the case. I was hanging out with my friends, going to dinners, TV show watch parties, doing normal adult things, but whenever I would tell people about this, I would be hit with, “Shouldn’t you be studying? How do you have time for all of that?” I decided it was not worth it to try to please everyone and explain myself, so I shut down and didn’t tell anyone outside of medicine what was going on in my life. To some degree I felt this fed that little monster even more, because I was not sharing all the extraordinary things I was learning. I was not sharing how I was learning to properly perform a physical exam on patients. I was not sharing the complex pathology behind diseases and how to treat them. I was not sharing how I was developing my communication skills with our standardized practice patients. I was not sharing how I was constantly being uplifted and supported by not only my classmates and friends, but also my professors and faculty advisors. Looking back, I think the main reason I decided to suppress and not discuss was because of my imposter syndrome. I felt that if I started to talk about a subject and got one thing wrong, then my months of learning proved nothing, showing that I didn’t belong in this field.
I had this grand idea in my mind of what my clinical years in school would be like, but the pandemic added hurdles and setbacks, which further contributed to my imposter syndrome. I’ve spent most of my third-year rotations online— 60 percent, to be exact—which has left me questioning if I really am ready to begin my residency. I’ve never witnessed a code, never rounded on in-patient care, my note writing skills are lacking, and frankly, I just have not had the experience I feel is necessary to graduate medical school. Thus, imposter syndrome is in full effect for me right now. I made it halfway through my third year when I realized I was just getting to my first full in-person rotation. Thankfully it was OB-GYN, the field I have fallen in love with and will be applying for in the 2022 residency match. I felt comfortable taking a gynecologic history, performing PAP smears, delivering placentas, assisting in the OR, and even having the incredible opportunity of catching a baby. Now, as I am nearing the end of my third year, I realized I had the expectation that I would know so much; however, I feel like I know so little and find myself looking forward to the day when it will all come together. When I look around at my other classmates, I realize I am surrounded by people who were at the top of their class, and while I am one of those people, I still find myself feeling inadequate. I still find myself wondering how they can connect the dots on their rotations and see the big picture. I still find myself wondering how they know what questions to ask. I still find myself wondering simply how they make it look so easy. The one benefit of spending most of my clinical time online is it has allowed me to have time for self-reflection. This year has allowed me to foster relationships with my friends in ways that would not have been possible with a full work schedule. This year has allowed me to make myself and my mental health a priority. Most of all, this year has shown me the amazing support system I have cheering me on every step of the way, especially during the hard times.
So, while I try my best to contain this little monster, there are days when it breaks free from the room it is kept in, and I sometimes am still unable to contain my feelings of being inadequate. When these days come, I’ve learned how to work through them. I remind myself of how far I’ve come to get here. I remind myself of the years of education and knowledge I have gained on this journey. I remind myself of the countless individuals who have supported me, encouraged me, and helped me on this path. I remind myself of what lies ahead, and while it is a long and arduous road, it is one I am happy to be on. Sacrificing the best years of my life to being confined to the library, where I am studying and absorbing an overwhelming amount of information, has been worth it to me. Some might ask why, and the only answer I can give is that whenever I am asked what I would do if I wasn’t in medicine, I honestly do not have an answer. So, this is how I lure the monster back into its room—by reminding myself of my worth, my perseverance, my triumphs, and my successes throughout this journey.
Part of me is curious if it is the competitive culture of medicine that contributes to imposter syndrome, or if it is the self-doubt we carry in ourselves because of how difficult the road is to becoming a doctor. My biggest question going into my fourth year is how do we combat this? How do we tell medical trainees that it is okay to have these doubts; that they are normal, and that you are still learning and absorbing everything around you? How do we tell them that medical school is hard, but you don’t have to endure it alone? I think the answer to these questions is acknowledging that everyone experiences imposter syndrome at least once, and it is okay to have these doubts. It is okay to take a step back and say, “Wait a minute, was that the right call? Was that the right diagnosis? Should I have treated my patient’s condition in a different way?” Acknowledging this monster allows us to not become complacent in our careers, ensuring we are doing the best job that we can. This is a big part of the reason I chose to pursue medicine—the constant educational and learning opportunities, the inability to ever become complacent in your job. My time in medical school has opened my eyes to the type of physician I want to be. I want to encourage and reassure the medical students I will one day work with that it is okay to not know the answer to everything. It is okay to ask questions out of curiosity, even if the answer is something that I view as common knowledge. It is okay to be nervous, it is okay to be scared, it is okay to simply not know things. Medical students are exactly what they are called: students. Here to learn, here to observe, and here to take in everything around them. They should be able to do this without fear of humiliation or being deemed incompetent. I want to be the type of resident that shows my students that I too suffer from imposter syndrome right there with them, and that with the right tools and strategies, it is possible to cage the monster.
My challenge to this generation of physicians is to look back on your time in medical school and think of a resident or preceptor that showed an interest in your education and made you feel like you belonged. Do you think you could have survived that rotation without their help? If you find yourself answering “yes,” I give my applause to you, but if you find yourself answering “no,” hold on to that thought, remembering it for when you have students of your own.
We don’t have to be alone on this journey. We should work together to normalize the conversation around the mental exhaustion medical school creates in individuals. We should work together to lift and encourage our peers. We should work together to ultimately say it is okay to have imposter syndrome, but here is how we can deal with it before it becomes something greater than we can contain.