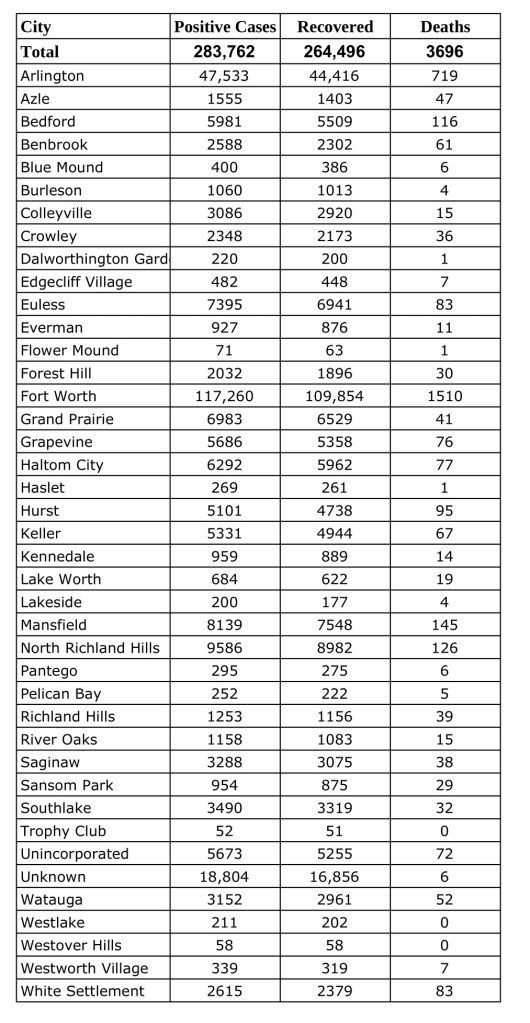
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Friday, August 13, 2021.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
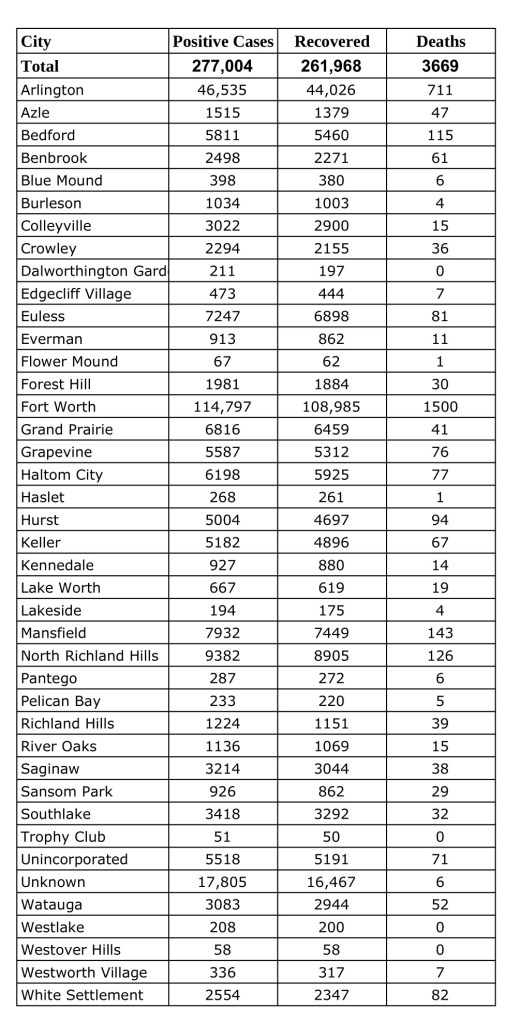
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Thursday, August 5, 2021.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
JPS Health Network is committed to helping ensure our community has the most up-to-date information about the COVID-19 pandemic. Due to an increase in the number of positive cases in Tarrant County, the Network is resuming a daily information phone line to provide facts about COVID-19 cases at JPS.
Starting today, information will be available as a recording updated every morning at 10 a.m. Callers can access the recorded message by calling 817-702-9500.
The recording will provide information including the number of inpatients who are undergoing treatment for COVID-19 at John Peter Smith Hospital. The phone line was in operation for about a year during the height of the pandemic, and was suspended in mid-June as the number of cases at the hospital dwindled.
This article was originally published in the July/August issue of the Tarrant County Physician. You can read find the full magazine here.
On the heels of the COVID-19 pandemic, pediatric suicide and mental health diseases are at all-time highs. According to the Centers for Disease Control and Prevention, suicide was the second leading cause of death for individuals between the ages of 10 and 34 in 2019.1 This research also noted that suicide rates have risen by 35 percent from 1999 to 2018 across the United States.1,2 With the arrival of the novel coronavirus pandemic and resulting social distancing, financial losses, and increased morbidity and mortality, we have seen an increase in the already high number of mood and anxiety disorders across all age groups. Children and adolescents have been especially impacted because of parental distress, social isolation, and difficulty adjusting to the virtual school environment. Many children with a pre-existing psychiatric diagnosis have experienced an exacerbation while others have experienced mental health symptoms for the first time, not knowing how to cope with the stress of their severely altered circumstances. Because the pandemic is currently ongoing, there is scarce research available to quantify the increase in mental health needs in the pediatric population due to COVID-19 and its restrictions.
Primary care providers and pediatricians have been on the front lines and often are the only point of contact for many patients before a suicide attempt. In 2015, researchers used National Institute of Mental Health-funded Mental Health Research Network data from 2009-2011 and found that 38 percent of patients who attempted suicide had made some type of healthcare visit within the week of the attempt, 64 percent within the month, and 95 percent within the year.3 This data shows us that primary care providers are integral in identifying and treating vulnerable patients that may not have access to psychiatric services.
Due to this urgent need for further pediatric mental health care services, the 86th Texas Legislature passed Senate Bill 11 in 2019, enacting the Child Psychiatry Access Network (CPAN), a telephone consultative service for primary care providers caring for children and adolescents with mental health needs. The caller will be greeted by a member of our team who will ask general questions about the call and can provide resources such as outpatient therapists, local partial hospitalization programs, and/or pediatric inpatient programs in the area if needed. If there are diagnostic questions or the need for support with treatment planning, consultation with a pediatric mental health provider can be arranged the same day.
Your local CPAN team wants to support you as you treat your pediatric patients’ mental health needs. The University of North Texas Health Science Center (UNTHSC) has partnered with John Peter Smith Health Network (JPS) to provide these services for Tarrant County and eight of the surrounding counties, including Parker, Wise, Cooke, Erath, Palo Pinto, Jack, Montague, and Clay. This service is free of charge with a response time of within five minutes for resourcing requests and 30 minutes for consultation with a child psychiatry provider. CPAN is ready to provide support to Texas primary care providers Monday through Friday from 8 am to 5 pm. Just call 1-888-901-CPAN, press 1 for North and North East Regions and press 1 again for the UNTHSC/JPS hub. You will be able to obtain needed resources or a consultation immediately. You can also contact the CPAN coordinator, Janet Thompson, at JThompso04@jpshealth.org to enroll, though enrollment is not required to make a call. We look forward to partnering with you to help your pediatric populations and their families.
2“Vital Signs: Trends in State Suicide Rates – United States, 1999–2016 and Circu stances Contributing to Suicide – 27 States, 2015.” Centers for Disease Control and Prevention. Centers for Disease Control and Prevention, June 10, 2019. https://www.cdc.gov/mmwr/volumes/67/wr/mm6722a1.htm?s_cid=mm6722a1_w.
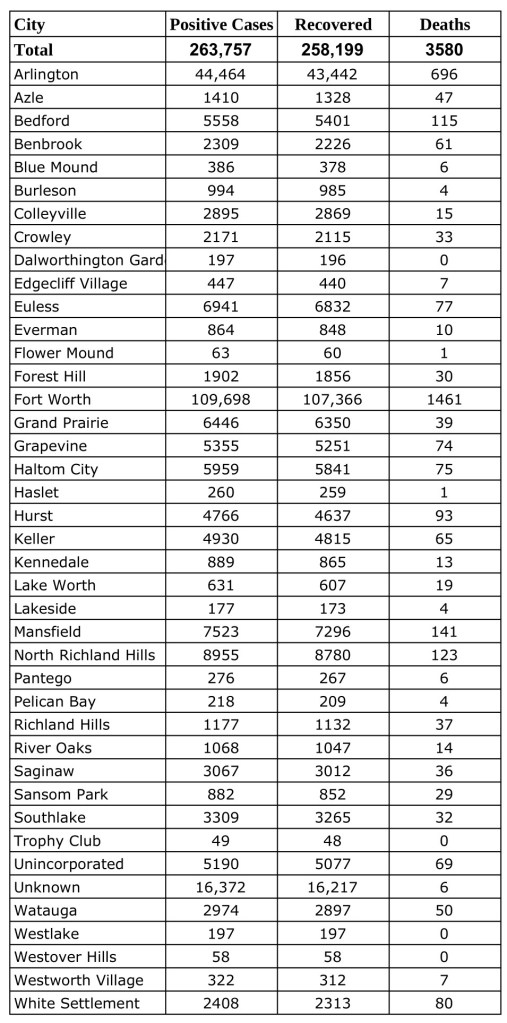
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Monday, July 26, 2021.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
Imagine your vision slowly getting worse, almost like a timer counting down. You aren’t sure of the colors on a traffic signal so driving becomes hazardous. Now, thanks to our generous donors and volunteers, 52-year-old patient, Ben, describes getting much-needed cataract surgery as “I feel like I was reborn.”
Ben can’t think of a better way to describe the moment he opened his eyes, and at last, could see clearly.
Previously, Ben, who is a kitchen manager, says his day-to-day life was a challenge.
“The restaurant where I work at is very fast paced, and I would get lost and behind due to my loss of vision. I couldn’t watch TV; I couldn’t see at night due to glare. I was scared to drive at night.”
Ben knew he needed help and needed to support his wife and daughter, but the cataract in his left eye continued to get worse, making his vision cloudy and unreliable. Ben went to Mission Arlington and was referred to an ophthalmologist to have the cataract removed, but he was unable to afford the surgery.
Project Access Tarrant County (PATC) works with other local nonprofits to refer patients to our team of volunteer doctors and clinics. Services are provided at reduced costs so patients like Ben are able to receive critical medical care.
Ben’s wife received treatments from PATC previously, so he reached us to us. After consultation with Dr. Tyler Moore, we coordinated with Baylor Surgicare who provided the venue for the procedure and Anesthesia Associates, Fort Worth Division of USAP, who provided the anesthesia care.
Ben and his family knew that it would be impossible to pay for the surgery without insurance and that cost would not be a barrier thanks to supporters to PATC.
Dr. Moore performed the surgery, and Ben couldn’t be more thrilled with the outcome.
“I couldn’t see if the light was red or green and I’d have to ask my wife for help, but now I no longer feel upset and mad that I couldn’t do what I wanted,” he says. “I can drive again comfortably. It’s totally different than when I was scared to drive.”
Donor support allows patients like Ben to resume normal life activities
“I am so thankful,” Ben says. “Project Access has changed my life.”
By Susan F. Franks, PhD, David Farmer, PhD, and Janet Lieto, DO The University of North Texas Health Science Center at Fort Worth Texas College of Osteopathic MedicineDepartment of Family Medicine and Osteopathic Manipulative Medicine, Department of Medical Education
Now more than ever, the most satisfying aspect of care—interacting with and helping patients—is overshadowed by the complexities of the modern-day practice of medicine. Your day may be more focused on interacting, coordinating, and making decisions with numerous ancillary people and various entities and stakeholders than the person before you who is seeking care. Coordinating your team and the administration of your practice demands independence, leadership, communication, and organizational skills. As the practice of medicine has evolved, you have progressively faced cumbersome EMRs, nuanced billing and coding expectancies, misinformation that patients get from the Internet, and varying organizational expectations. The on-going evolution of practicing medicine places further demands on the skills of flexibility and stress tolerance.
But perhaps the most subtle transformation in medicine is the increased necessity of creating and maintaining interpersonal relationships. The traditional circle and hierarchical approach of running a practice in the past has transformed into collaborative partnerships with patients, families, colleagues, consultants, administrators, and other key stakeholders. At times you are required to be a team leader, at times a team member. You must still attend to patients and provide expert counsel and education, all the while dealing with interruptions, personal agendas, and a vast array of different communication and personality styles. All your responsibilities are expected to be fulfilled with confidence, respect, professionalism, and above all, treatment effectiveness and a gracious attitude of sharing in successful outcomes, but while still bearing the burden of responsibility when things fall short. You must approach each day with an appropriate balance of assertiveness and impulse control, objectivity and optimism, and emotional expression and empathy.
The twenty-first century physician is immersed in a continually evolving interprofessional, team-based environment where medicine is delivered under an often-fragmented system of care.1 The traditional patient-physician dyad has expanded to encompass a wider net of individuals, all of whom must be integrated to meet clinical outcomes, patient satisfaction, and fiscal demands. Added to this is the increasing awareness of inequities in medical care, an explosion of public access to medical information and misinformation, cost-control strategies, and the politicization of medicine, adding enormous complexities to the primary task of simply caring for the patient sitting before you.
Never has the practice of medicine and the expectations of the people involved in every aspect of it been more dependent on the social and emotional skills of the physician than they are today. This is a world that the doctors of the future must be prepared to enter. A world where cognitive intelligence is not the only predictor of success. A world that depends on the emotional intelligence of the physician for the system to function effectively.
What is Emotional Intelligence?
Emotional intelligence (EI) is a set of social and emotional skills that collectively establish how well we perceive and express ourselves, develop and maintain social relationships, cope with challenges, and use emotional information in an effective and meaningful way.2 EI skills are also associated with the development of empathy, self-awareness, motivation, emotional control, and effective communication.3,4 Compared to people with low EI skills, individuals with high EI perceive, understand, and manage emotions better, are less likely to engage in problematic behavior, and have more positive social interactions.5 Individuals with high EI skills also report lower perceived stress, are highly adaptable, and are more successful in leadership.6
Never has the practice of medicine and the expectations of the people involved in every aspect of it been more dependent on the social and emotional skills of the physician than THEY ARE today.
Several models of EI have been introduced, but all are founded on four related fundamental skills: self-awareness, self-management, social awareness, and social management.7 To best manage your behavior, you must first be aware of your emotional states. People with low self-awareness may have difficulty distinguishing between the nuances of feelings, for example the difference between irritability and anger. They may display emotions that are out of proportion to the situation and have difficulty recognizing that their response may not be appropriate. This places them at risk of not being able to maintain mutually respectful relationships, tolerate frustration, be a collaborative member of a team, or create an environment of psychological safety expected from a good leader. Interestingly, 95 percent of people believe that they are emotionally self-aware, but only 10–15 percent are.8 In contrast to earlier beliefs, we now know that the skills of EI can be taught and improved.9
Emotional Intelligence in Medical Education
Many students entering medical school do not have mature development in interpersonal and communication skills (ICS), particularly in dealing with patients and interprofessional relationships. Competency in ICS is woven throughout Entrustable Professional Activities (EPAs) that are being taught in medical schools. As teamwork becomes increasingly important in medical care and decision-making, physicians of the future need to be poised to collaborate so they can achieve the best patient outcomes. Teams with high EI can create a shared vision and achieve results through mutual trust that is fostered through empathy, flexibility, and other key social and self-regulation skills. Furthermore, EI has been found to predict psychological well-being, life satisfaction, and success in collaborations and interpersonal relationships. It enhances higher level thinking through the development of advanced cognitive strategies used to understand and respond to others, thereby improving diagnostic and therapeutic decision making.3,10 Alarmingly, when unattended, EI may diminish throughout medical training, contributing to reduced resiliency and the increased number of residents entering the profession feeling burned out.11,12 EI is now more widely considered to be an essential skill set for medical student development.13
At the Texas College of Osteopathic Medicine (TCOM), we promote the progressive development of emotional and social self-awareness by having medical students reflect on their EI skills and establish targets for growth. They work with an accountability partner to identify progress and areas needing improvement. It is often during clerkships that the social, emotional, and behavioral skills associated with EI are most observable and can provide a deeper understanding of why a student might be experiencing difficulties. Preceptors and residents give feedback on professionalism, teamwork, and interpersonal communication, helping students explore their use of EI skills. For example, a student who is overoptimistic may miss preceptor comments and clues indicating a need for improvement. They are then caught off guard at the summative performance evaluation when they rate lower than they anticipated. Progressive guidance in targeted EI skill growth can help students manage pertinent skills effectively.
In the TCOM curriculum, we integrate educational activities to improve the skills of EI. We start with a baseline assessment during the first week of their Medical Practice class using a well-established self-report assessment of EI called the EQi-2.0.®14 A student’s results are explained, and the student is introduced to the basics of EI and given a framework that emphasizes how EI skills are applied to patient care, teamwork, leadership, and personal well-being.
Activities to develop EI are strategically integrated into our Medical Practice course curriculum, which teaches students to gather health information and perform appropriate physical examinations, acquire competency in Osteopathic Manipulative Medicine, and apply knowledge and skills to patient encounters. Topics begin with a focus on self-care and the use of the EI skills of flexibility, optimism, and stress tolerance to aid in adjustment to the rigors of medical school. Students later examine the role of emotional self-awareness, self-expression, and empathy as applied through standardized patient encounters. As students engage in small-group learning, EI skills of teamwork and leadership are introduced, and students rotate leading their team. In one particularly cogent activity, students each select a respected faculty physician as a model of emotionally intelligent leadership.
When students approach Year 2 board exams, we advance their stress management skills toward peak performance, and they evaluate their balance of optimism and reality. In the Professional Identity and Health Systems Practice Course, EI aids students in the development of professional identity and in management of that identity as they contemplate how they will fit into the healthcare system as an osteopathic medical student, a resident, an attending, and a life-long learner. EI is reassessed prior to the clerkship year to identify their progress and areas in need of further improvement. It is then revisited in the Family Medicine Clerkship, with a focus on patient care and interprofessional collaboration. Throughout the integrated EI curriculum, evidence-based principles of social learning and cognitive-behavior strategies help promote lasting change.
Conclusion
EI development can help physicians navigate the intra- and interpersonal complexities of the practice of medicine in areas not directly related to technical skill or medical knowledge.13,15 EI is a significant part of clinical competence and is tied to increased patient satisfaction, because it affects a physician’s ability to understand and relate to emotional barriers that patients experience.16,17 In support of the patient, EI can also increase the effectiveness of the healthcare team. In support of the healthcare team, EI can help reduce burnout through the development of resiliency, psychological safety, and mutual support. A focus on personal well-being can include EI development for improved resiliency, personal relationships, and work-life balance. With this understanding of the nature of EI, educational strategies are being utilized to prepare high EI physicians for the challenges of the twenty-first century.
4Orak, Roohangiz Jamshidi, Mansoureh Ashghali Farahani, Fatemeh Ghofrani Kelishami, Naima Seyedfatemi, Sara Banihashemi, and Farinaz Havaei. “Investigating the Effect of Emotional Intelligence Education on Baccalaureate Nursing Students’ Emotional Intelligence Scores.” Nurse Education in Practice 20 (June 23, 2016): 64–68. https://doi.org/10.1016/j.nepr.2016.05.007.
5Mayer, John D., Peter Salovey, and David R. Caruso. “Emotional Intelligence: Theory, Findings, and Implications.” Psychological Inquiry 15, no. 3 (2004): 197-215. http://www.jstor.org/stable/20447229.
6Chun, Kyung Hee, and Euna Park. “Diversity of Emotional Intelligence among Nursing and Medical Students.” Osong public health and research perspectives vol. 7,4 (2016): 261-5. doi:10.1016/j.phrp.2016.06.002
7Bradberry, Travis, and Jean Greaves. Emotional Intelligence 2.0. San Diego, CA: TalentSmart, 2009.
8Eurich, Tasha. Insight: The surprising truth about how others see us, how we see ourselves, and why the answers matter more than we think. New York, NY: Penguin Random House, LLC. 2001.
10Johnson, Debbi R. “Emotional Intelligence as a Crucial Component to Medical Education.” International Journal of Medical Education 6 (2015): 179–83. https://doi.org/10.5116/ijme.5654.3044.
11Dyrbye, Liselotte N., Colin P. West, Daniel Satele, Sonja Boone, Litjen Tan, Jeff Sloan, and Tait D. Shanafelt. “Burnout Among U.S. Medical Students, Residents, and Early Career Physicians Relative to the General U.S. Population.” Academic Medicine 89, no. 3 (2014): 443–51. https://doi.org/10.1097/acm.0000000000000134.
12Hansell, Maggie W., Ross M. Ungerleider, Courtney A. Brooks, Mark P. Knudson, Julienne K. Kirk, and Jamie D. Ungerleider. “Temporal Trends in Medical Student Burnout.” Family Medicine 51, no. 5 (2019): 399–404. https://doi.org/10.22454/fammed.2019.270753.
13Parks, Mitchell H., Chau-Kuang Chen, Christina D. Haygood, and M. Lisa McGee. “Altered Emotional Intelligence through a Health Disparity Curriculum: Early Results.” Journal of Health Care for the Poor and Underserved 30, no. 4 (2019): 1486–98. https://doi.org/10.1353/hpu.2019.0091.
14Multi-Health Systems, Inc. The Emotional Quotient-Inventory 2.0® (EQi-2.0®). MHS Beyond Assessments. https://mhs.com/.
15Coskun, Ozlem, Ilkay Ulutas, Isıl Irem Budakoglu, Mehmet Ugurlu, and Yusuf Ustu. “Emotional Intelligence and Leadership Traits among Family Physicians.” Postgraduate Medicine 130, no. 7 (2018): 644–49. https://doi.org/10.1080/00325481.2018.1515563.
17Wagner P.J., Ginger C. Moseley, Michael M. Grant, Jonathan R. Gore, ChristopherOwens. Physicians’ emotional intelligence and patient satisfaction. Fam Med. 2002 Nov-Dec;34(10):750-454. PMID: 12448645.
All of these physicians are members of the Tarrant County Medical Society.
Tilden L. Childs III, MD, a diagnostic radiologist in practice for 41 years; reelected to the TMA Council on Legislation.
Shanna M. Combs, MD, an obstetrician-gynecologist in practice for nine years; appointed chair of TMA’s Committee on Membership and reappointed to the committee, and reappointed as a consultant to TMA’s Committee on Reproductive, Women’s and Perinatal Health.
Cheryl L. Hurd, MD, apsychiatrist in practice for 19 years; reappointed as a consultant to the TMA Committee on Physician Health and Wellness.
R. Larry Marshall, MD, a rheumatologist in practice for 32 years; appointed to TMA’s Committee on Continuing Education.
G. Sealy Massingill, MD, an obstetrician-gynecologist in practice for 32 years; appointed as a consultant to the TMA Council on Science and Public Health, and reappointed as a consultant to TMA’s Committee on Reproductive, Women’s, and Perinatal Health.
Matthew M. Murray, MD, a pediatric emergency physician in practice for 31 years; reappointed to TMA’s Committee on Health Information Technology.
Stuart C. Pickell, MD, an internist and pediatrician in practice for 21 years; elected to TMA’s Council on Medical Education, and reappointed as a consultant to the TMA Council on Health Service Organizations.
Drew Elizabeth Rainer, MD, an obstetrician-gynecologist in practice for four years; elected to TMA’s Council on Medical Education.
Angela D. Self, MD, an internist in practice for 19 years; reappointed to TMA’s Committee on Patient-Physician Advocacy.
Linda M. Siy, MD, a family physician in practice for 28 years; reelected to TMA’s Council on Legislation.
TMA is the largest state medical society in the nation, representing more than 55,000 physician and medical student members. It is located in Austin and has 110 component county medical societies around the state. TMA’s key objective since 1853 is to improve the health of all Texans.
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Monday, July 12, 2021.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Tuesday, July 6, 2021.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.