Physicians found new flexibility in prescribing controlled substances via telemedicine during the COVID-19 pandemic.
Now that the public health emergency is ending, the Drug Enforcement Administration (DEA) has proposed new rules for prescribers it says could preserve some of those flexibilities “with appropriate safeguards.”
Among other things, the new rules – if finalized – would allow physicians and health care professionals to prescribe, without a face-to-face visit, a 30-day supply of Schedule III and Schedule IV non-narcotic controlled drugs, after which an in-person follow-up would be needed for any refill. This class of drugs is the least likely to result in drug abuse, according to DEA. The proposal also would allow for prescribing a 30-day supply of buprenorphine to treat opioid use disorder without an in-person evaluation or referral.
“Improved access to mental health and substance use disorder services through expanded telemedicine flexibilities will save lives,” Department of Health and Human Services Secretary Xavier Becerra said in the announcement. “We still have millions of Americans, particularly those living in rural communities, who face difficulties accessing a doctor or health care provider in person.”
The agency emphasized that the rules do not affect telehealth services that do not involve controlled substance prescriptions. The Texas Medical Association is reviewing how the proposed regulations could interact with other federal and state regulations, says Shannon Vogel, TMA’s associate vice president of health information technology.
DEA has released summaries for both healthcare professionals and patients explaining how the proposed rules would affect prescription practices.
“This is a very good thing that they’re doing and a necessary thing” for access to care, said Mesquite pain management specialist C.M. Schade, MD, a former president of the Texas Pain Society.
Before the pandemic, physicians were limited in their telemedicine prescribing ability by the Ryan Haight Online Pharmacy Consumer Protection Act of 2008, he says. The act requires physicians to conduct at least one in-person medical evaluation of the patient before prescribing a controlled substance by means of the “internet,” which is defined to include telehealth.
“COVID did great things for telehealth, and one of them was breaking through the Ryan Haight Act,” Dr. Schade said.
Some policymakers and behavioral health advocates have expressed concern, however, that patients who need continuous medication therapy may have challenges obtaining an in-person visit within 30 days.
The rules were proposed on Feb. 24 and public comments are due on March 31. The agency has no set timeline for publishing the rules, though it is likely that will come before the PHE ends on May 11.
Physicians with questions and comments about the DEA changes or relevant state regulations can contact Ms. Vogel.
The Centers for Medicare & Medicaid Services (CMS) recently posted the 2023 Medicare Physician Fee Schedule, which takes effect Jan. 1 and brings with it a mixed bag of consequences for physicians.
The Texas Medical Association continues to fight certain elements of the final rule, including a nearly 4.5% physician pay cut and additional changes to the already-byzantine Merit-Based Incentive Payment System (MIPS). But the association also celebrates the victories in the regulation, including expanded cancer coverage and reduced administrative requirements.
TMA experts discuss the key updates from the final rule in the new, on-demand 2023 Medicare Update webinar. It is free to TMA members, and you can earn 1 AMA PRA Category 1 Credits™ that may count as ethics credit.
A physician paycut and other concerns
The 2023 fee schedule lowers the conversion factor that determines physician payments by 4.47% compared with the 2022 formula, leaving many physicians concerned about their bottom line. Barring intervention by Congress, the cut would be one of many to take effect next year, including a sequester cut and other reductions mandated by law, totaling 8.5%.
Robert Bennett, TMA vice president of medical economics, is hopeful Congress will act to avert the cuts, but he cautions lawmakers could wait until January to do so retroactively.
“There are so many issues being debated in Washington, D.C. right now,” he said during the event. “I’m worried this is a back-burner issue for them.”
TMA urges members physicians to download its Medicare Payment Cuts Toolkit, which outlines ways to press lawmakers to intervene.
In the meantime, TMA joined the American Medical Association and others in organized medicine in writing to Congressional leadership on Dec. 1.
“Put simply, the cost of Congressional inaction is an across-the-board cut that will further amplify the financial hardship physician practices are already facing while inhibiting Medicare from delivering on its promises to seniors and future generations,” the signatories wrote.
TMA also has joined forces with AMA and scores of state and specialty medical societies to push for comprehensive Medicare physician payment reform. Such a long-term fix would prevent the need for physicians to lobby their representatives multiple times a year about impending pay cuts – or risk their practice viability.
As in previous years, the fee schedule also includes changes to MIPS, one of two pathways under Medicare’s Quality Payment Program. CMS says the changes focus on MIPS Value Pathways (MVPs) – a new, optional reporting framework set to debut in the 2023 performance year – and limit adjustments to traditional MIPS in an effort to spur participation in MVPs.
TMA has repeatedly asked CMS to reconsider MVPs and to focus instead on the development of voluntary, physician-led alternative payment models (APMs). Still, Mr. Bennett encouraged physicians who participate in MIPS to consider MVPs, which he said function as a hybrid between fee-for-service MIPS and value-based care APMs.
CMS is hosting a webinar on Dec. 14 from 1-2 pm CT about MVPs, including its rollout and how physicians can submit an MVP candidate for consideration. You can register for the virtual event via Zoom.
Fee schedule gains
Despite these concerns, the 2023 fee schedule includes meaningful gains when it comes to the Medicare Shared Shavings Program (MSSP), evaluation and management (E/M) coding and payment, certain pandemic-era flexibilities, electronic prescribing of controlled substances, and colorectal cancer screening.
TMA welcomes some of the changes to MSSP, which its experts say could reduce barriers to participation. For instance, CMS will make advanced investment payments available to certain new accountable care organizations, which they could use to purchase the technology and data management resources and to hire the care coordinators necessary to participate in the program.
At the same time, TMA has asked CMS to consider phasing in – and even limiting – recoupment of any advance funding to encourage long-term participation as well as providing new opportunities to engage specialists in Medicare’s value-based programs.
CMS also will institute significant changes to E/M coding in the new year, heeding recommendations from TMA and AMA. These include simplified documentation requirements and increased payment for services provided at several sites, including hospitals, emergency departments, nursing homes, and patient’s homes.
Although this is a positive development, Mr. Bennett said these payment increases contributed to the 4.47% reduction in the conversion factor, given federal budget neutrality requirements.
CMS also delayed the implementation of a confusing policy related to split (or shared) visits, which determines who should bill for a shared visit. The fee schedule maintains the existing guidelines, and CMS will revisit the issue in its 2024 fee schedule.
In addition, the 2023 fee schedule offers some guidance on telehealth coverage once the federal public health emergency (PHE) related to COVID-19 ends. With it, CMS has extended certain telehealth flexibilities for 151 days after the PHE ends, including allowing:
Practices to use non-HIPAA complaint telehealth platforms; and
Medicare patients to access telehealth services anywhere, including at home, and via audio-only options, among other changes.
This aligns with Congress’ action in March, when it passed a spending package extending these same flexibilities for 151 days after the PHE ends.
Shannon Vogel, TMA associate vice president of health information technology, said physicians should anticipate making changes once the PHE and the 151-day grace period end, such as phasing out non-HIPAA compliant telehealth platforms and audio-only telehealth services. But she added that they still have time to do so.
“At this point, we feel pretty confident that the PHE will probably extend through about mid-April or so,” she said, which would put the end of the grace period in mid-September.
The PHE is currently slated to expire in January. However, the federal government has said it will give states 60-days’ notice of its end, a deadline that came and went in mid-November. Although the government hasn’t announced a new deadline, it previously has extended the emergency declaration in 90-day increments.
As recommended by TMA and others in organized medicine, CMS will delay until 2025 financial penalties for physicians who don’t electronically prescribe controlled substances. Although TMA supports this move, it has pushed CMS to go further by scrapping such penalties altogether, especially for those practices that do not do high volume e-prescribing.
Starting next year, Medicare patients also will benefit from expanded coverage of colorectal cancer screening tests, following advocacy by TMA and others in organized medicine. CMS gradually will reduce coinsurance payments for Medicare patients who undergo unplanned colorectal screening tests until 2030, when the federal agency will waive such copayments altogether.
TMA endorsed this policy change in its comment letter, writing that it would “reduce the financial burden facing Medicare [patients] whose screenings result in a diagnostic procedure” as well as “promote utilization of colorectal cancer screenings that save lives.”
Dr. Combs giving her first speech as the 2022 TCMS president
And just like that, my year as the Tarrant County Medical Society president is nearly over. It has been a pleasure to serve in this role, and while my time is almost up, I wanted to look back over the past year.
My time started at the end of last year during an early reprieve from the COVID pandemic. The Gold-Headed Cane and President Installation was our first in-person event since the start of COVID. It was an amazing night of getting to see old colleagues and meet new ones. It was also amazing to have four female physicians being honored in one night; it was great to share the evening’s celebration with Drs. Susan Bailey, Teresa Godbey, and Angela Self.
Being inducted by Dr. Angela Self as the new TCMS president
Unfortunately, the year took a step back due to the COVID pandemic, and we once again had to change to a virtual meeting for the TMA Winter Conference. As we have done multiple times during the pandemic, we were able to pivot and carry on. Locally, our TCMS leadership came together to promote fellow physicians to seek out positions at TMA.
As we moved to April, we started to see light and were finally able to hold TexMed in person, the first time since 2019. The best part of the meeting was seeing the inauguration of our own Gary Floyd as TMA president. Moving into summer, we were able to have a Women in Medicine event where we gathered for some much-needed stress relief making bath bombs. While we were not all successful at making the bath bombs, we had a great time gathering again in person.
Making bath bombs at the Women in Medicine event
When the Dobbs decision came out in June, I had multiple opportunities to speak with local and national media about the importance of the patient/physician relationship, and how this decision has many far-reaching implications in medicine. I will continue to work on advocating for doctors and patients to make their own medical decisions without intervention from outside forces.
At the Young Physicians Mixer
During July, I had the privilege to welcome our new Tarrant County medical students from the Texas College of Osteopathic Medicine and the Anne Burnett School of Medicine at TCU to TCMS and the world of organized medicine. It was refreshing to meet with these young students and to cheer them on as they begin their journey to having the greatest job on the planet: being a physician.
As we moved into the fall, we had another opportunity to gather again at the TMA Fall Conference. We are slowly finding our way through this COVID pandemic, returning to some form of normalcy. While I cannot quite say it seems to be over, as this has been said too many times before, we continue to find a way through.
Speaking to the incoming class of medical students
While my tenure as TCMS president may be coming to an end, I will continue to contribute to the work of our county, state, and national medical societies. If I have learned anything over the past year, it is that we must be at the table and part of the discussion; otherwise, people who don’t practice medicine will continue to try to tell us how to do our job. We have worked too hard to become physicians to allow others to practice medicine for us, and it isn’t in the best interest of our patients or our vocation – the work that still is, despite so many challenges, the best job on the planet.
Linda Siy, MD, of Fort Worth, Texas, has been awarded the highest honor among Texas family doctors by the Texas Academy of Family Physicians. She was named the 2022 Texas Family Physician of the Year during TAFP’s Annual Session and Primary Care Summit in Grapevine on Oct. 29. Each year, patients and physicians nominate extraordinary family physicians throughout Texas who symbolize excellence and dedication in family medicine. A panel of TAFP members chooses one as the family physician of the year.
“It truly is an honor to join the ranks of those who have received this distinction, and I’m very humbled to be considered with those distinguished colleagues who previously were Family Physicians of the Year,” Siy said as she accepted the award.
Siy has been a family physician for over 30 years, and currently practices at John Peter Smith Health Network at the Northeast Medical Home in Tarrant County, a practice she’s been a part of since 1995. She is also faculty at the University of Texas Southwestern School of Medicine, the University of North Texas Health Science Center/Texas College of Osteopathic Medicine, and the Texas Christian University Burnett School of Medicine.
Throughout her years in organized medicine, Siy has served on many committees and councils for both TAFP and the American Academy and has been president of the TAFP Foundation since 2017. She serves on the Acclaim Multispecialty Group’s Physician Board of Directors, and previously served as president of the Tarrant County Medical Society and TAFP’s Tarrant County chapter.
Siy has spent her career in medicine treating her loyal and multi-generational families of patients, many of whom are underserved, suffer from housing and food insecurity, and struggle with mental health and substance abuse. Many of her nominators mentioned her willingness to speak up and ask the questions others are too afraid to ask, as well as her dedication to teaching the next generation of family physicians.
“I think what’s kept me in the game for so long at the place where I work now are those rewarding relationships with your patients, with your staff, with your colleagues,” Siy said of her career in family medicine. “It’s really not a job. It’s a calling.”
This article was originally published in the May/June issue of the Tarrant County Physician. You can read find the full magazine here.
I once wrote about my hopes for life after medical school. I would imagine my office decor, my conversations with patients, the time I would spend coordinating their care. The thoughts were all happy and gave me hope when the dark days of medical school cast a shadow over my upbeat mood, when classes took me down the road of insomnia and gave me a near flat affect from studying more than 12 hours a day during exam time. I guess we all looked like zombies immediately before and after our exams, and some even had the fragrance.
Once a girlfriend came to visit me and she stayed at a hotel on the beach. I discovered the pleasure of sitting and enjoying a piña colada and having zero thoughts of gluconeogenesis or small, slow-conducting fibers (protopathic). Denise, the Coyaba hotel, and a piña colada were all little lights for a med student who was over 2,000 miles from home.
There are times during my professional life that I once again feel like I’m over 2,000 miles from home. Denise is now married and living in Ohio. Piña coladas have way too many calories. The Coyaba hotel would require more PTO than I’m able to take. I’m sitting at my dining room table as I write this because stepping back into the office would make me feel like I’m still at work. I started to take an evening walk but turned around when a close friend told me how much my article sucked (the one you’re not going to read). He didn’t actually say that it sucked; he just pointed out how opposite of uplifting or encouraging it was and said, “It’s not your best work.” Thank you, “D,” for your honesty.
Why would I not be the happiest person you could meet? I have a great job. I am happily single and able to go out and meet a girlfriend for coffee any time I want. I see my beautiful daughter on a regular basis (who is working, doing well in school, and enjoying her youth by spending time with her close friends). My mom survived a hospitalization that nearly took her life in 2013 and has never smoked again (I had taken her home on hospice ten days after she was admitted). Heck, I barely have enough bills to qualify as debt. I should be dancing around the whole Grapevine/Colleyville area. But I’m not.
The strange thing about being there for everyone else is that you sometimes forget to keep a little piece of yourself to enjoy—you just give it all away. Yes, this is a “me” problem. I am the one who picks up the phone when I know the person calling is going to vent for the next 30 minutes, but after 20 years of friendship, you make an effort to still “be there” because that’s what friends do. When your very best friend calls and frantically asks for prayer because the vet is coming to put their horse down (which happened two days ago), how do you not take that call? When your mom wants to tell you about a grandkid she’s concerned about and says the stress is overwhelming, are you going to hang up on her? Another friend tells you they are really concerned because they are still having fatigue and shortness of breath since their heart procedure—and this is one of your health-conscious friends. How can you not feel that? Then there is the job that you love doing, but sadly you do it for 12 hours many days. I find myself on long walks, asking, “Am I missing something?” I wonder if there are elderly patients that I could be helping, or if I’m not fulfilling my calling by now being on the “administrative” side of Medicine.
Long walks, good coffee, and two cats have replaced Denise, the Coyaba, and even the piña colada. As I walk along, I play music from the 80s and 90s and look at all of the different trees—I love the long needle pines the best, they look and smell good. I see the cardinals and the other birds flying around and admire how they know the meaning of commitment. On the weekends I spend hours at the coffee shop with the same few people I’ve been meeting there for years (none of us got COVID-19, and almost everyone is getting vaccinated). They give me a special discount at Buon Giorno, just don’t tell anyone. What? They give everyone that same discount for bringing their thermal mug? I look up at the stars and try to find the big dipper, but I live in Grapevine and, you know, light pollution. I run a hot bath and sit there until it’s barely warm. Netflix holds many fond memories from my COVID-19 nights: Shtisel, Sex and the City, The Crown, Girlfriends . . . I really do make the most of each day and try to laugh as much as I can. It’s just been hard to laugh lately, and I wanted to share in case someone else is also having a hard time laughing, or sleeping, or even folding the laundry.
We are the ones who are there for everyone else. Who is there for us? Though my friends and family can drain the very life force from my body, I want you to know that I am here for you. You have sacrificed so much for others, and your colleagues see you. They care even though you thought they didn’t like you. I am struggling a bit these days, as I suspect many of us are after the year we’ve been through.
Perhaps this is just my COVID-19 carb crash, but I am ready for this season to end. I am praying; I like to pray. I am even going to church on occasion . . . not that I care for going to church. But my faith has always seen me through the most difficult of times, and I once again find myself reading Joshua 1:9, knowing that He will be with me wherever I go. I am going to put that and a few other verses on the wall behind my laptop as a reminder that He is always with me. I have friends who do not share my faith, my politics, or my taste in music, but we do share the need to connect, to laugh, and to be heard. Thank you for reading my article and for being one of the lights in a sometimes dark place. Call me any time at 817-798-8087 (text first if you actually want me to pick up). We’re all walking through this—let’s do it together.
This was published by Texas Medical Association. You can read the original version here.
This is not business as usual. The COVID-19 pandemic has affected physician practices both clinically and economically.
You may already have made changes in how you care for patients, such as utilizing telemedicine in place of in-person visits.
For a big picture perspective, Catalyst Health Network, a clinically integrated primary care network, has created a financial workbook you can download that calculates the effect a decrease in patient encounters and revenue has on your practice.
You also can make adjustments in operating expenses that can keep your practice’s finances healthy.
According to the Medical Group Management Association (MGMA) benchmark data, staff salaries and building occupancy are the two largest expenses in a physician practice. Staffing alone typically accounts for 25% of total operating expenses, and leases account for another 6% to 10%.
However, these can be difficult sums to change: We want to support our staff, and we need to maintain an office space.
There are other fixed expenses, like insurance payments, that may be deferred but not necessarily adjusted. However, there are some things you can do:
Lease: Contact your landlord to discuss a deferment of monthly payments. If you are in your renewal period, negotiate a deal that includes a lower payment and/or deferment for the first few months of the new lease.
Staffing: There are a few options like layoffs or furloughs, but be sure to consider your future funding needs as your decision could have an impact on loan forgiveness. If you furlough, you still need to pay for benefits. Furloughed staff are eligible to apply for unemployment as well. You also can consider rotating staff if you have patient care or billing needs to fulfill.
Supplies: Stop automatic orders so you can have more control over which medical and office supplies you pay for. Consider joining a group purchasing organization (GPO) for pricing considerations if you are not already a member.
Equipment leasing: Contact your vendors for any assistance they could provide during the current crisis. Your vendors might be able to defer or lower payments for a period of time. Evaluate use of equipment to determine if it is truly necessary to your practice. If not, return it and eliminate a payment.
Subscriptions: Suspend any magazine or other unnecessary subscriptions.
Shredding/Biohazard/Laundry Services: Suspend services you are currently not using.
On the income side, Catalyst Health Network also has created a tool that compares the Small Business Association’s (SBA) lending options: Express Loan, the Paycheck Protection Program, and Economic Injury Disaster Loans. The tool has information on when and where to apply, the qualification requirements, and other pertinent details.
Remember, you can find the latest news, resources, and government guidance on the coronavirus outbreak by visiting TMA’s COVID-19 Resource Center regularly.
TCMS is organizing a Physician Task Force to supplement community hospitals at this critical time. We need your support – please join this effort on the front lines of the coronavirus pandemic.
If you are interested in volunteering, fill out this form and contact Brian Swift at (312) 330-4894 or bswift@tcms.org.
Moncrief Cancer Institute has teamed up with Carter BloodCare to host a blood drive on Sunday, March 29 from 9 a.m. to 3 p.m.at the Rosedale Donor Center. This is considered an essential activity and is approved by the City of Fort Worth. We need the community’s help to keep the blood supply ready.
Sunday, March 29 from 9 a.m. to 3 p.m Carter Bloodcare: Rosedale Donor Center 1263 W. Rosedale Fort Worth, TX 76104
Click this link to sign up – must pre-register to honor social distancing! On the day of the blood drive, donors will receive a link to a short, online questionnaire to complete.
Carter BloodCare donors help provide blood for 90% of the hospitals in North, Central, and East Texas, and their supply has decreased due to drives/appointments being canceled. Blood is needed for cancer patients, transplant recipients, heart surgery, and trauma. Giving blood is safe, and Carter BloodCare is taking all precautions to ensure the safety of the donors. The team wears personal protective equipment throughout the entire blood drive and exceeds all FDA guidelines.
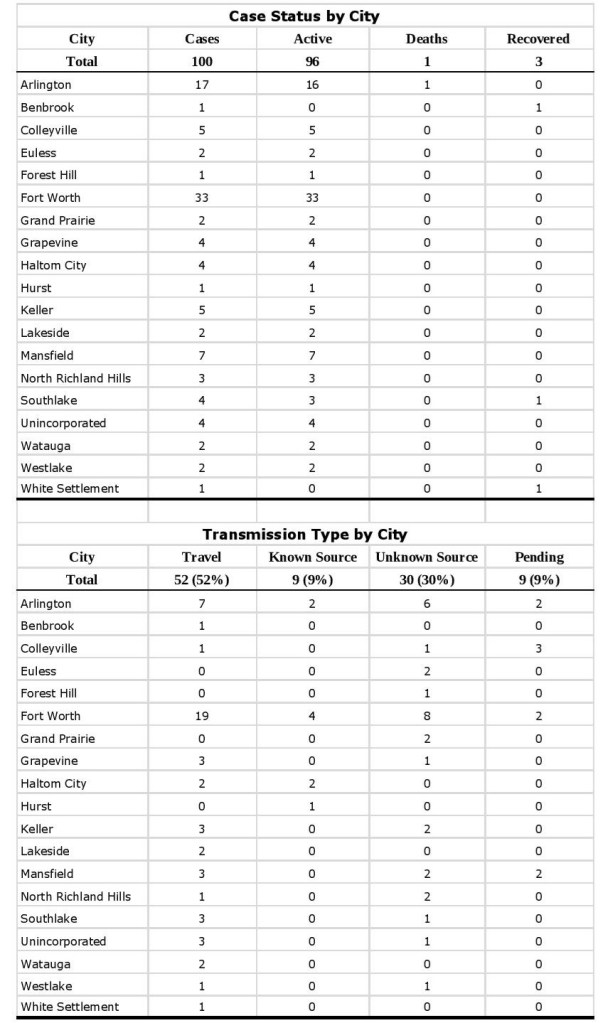
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Thursday, March 26, 2020 at 11:45 a.m.Find more COVID-19 information from TCPH here.
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County, updated Wednesday, March 25, 2020 at 11:30 a.m.Find more COVID-19 information from TCPH here.