Antonio Igbokidi, a second-year medical student at TCU School of Medicine, brings Black men together to discuss mental health at a Fort Worth barbershop.
“It’s all about figuring out ways to get men of color to have raw, vulnerable and organic conversations about mental health,” Igbokidi said. “Figuring out how to destigmatize and demystify mental health.”
Dr. Dixon is a psychiatrist with his own private practice in Fort Worth. He helped guide the discussion among the two dozen of men that came to the barbershop.
“It’s always fun to be in the classroom but to see one of my students actually out in the community doing some amazing work connecting people is amazing,” Dr. Dixon said.
For two hours, Igbokidi and Dr. Dixon, led the discussion where the participants talked freely about issues among Black men, young and old, in their community. The group shared their thoughts on crime, love, relationships, fatherhood, jobs and more.
“As a psychiatrist I’ve heard a lot in my day,” Dr. Dixon said. “But today was really poignant because it came from Black men and people who look like me. I’m really glad that they were felt safe enough to be in this space and share and that they trusted me with that honesty.”
Igbokidi also collaborated with the Black Heart Association to offer free screening for cardiovascular disease for anyone attending the session. Michael and Tara Robinson, co-founders of the Black Heart Association, were happy to be a part of something to help ease the hearts and minds of Black men.
“Everything flows through the heart whether it be mental or emotional,” Michael said. “As African American men we’re raised in a culture where we’re taught to be strong. Even as young boys there’s not a space for us to have safe conversations and be vulnerable.”
The men were able to get their glucose levels, cholesterol, blood pressure and risk of heart disease checked. The Black Heart Association has a mobile heart center where they go to barbershops, and other places, around Tarrant and Dallas Counties and offer free screenings for heart disease.
“We know that mental health plays a part in heart disease so this event was like the perfect marriage between what we do and what Toni is doing,” Tara said.
Igbokidi plans to continue the mental health sessions with his next stop being in the historic Stop 6 neighborhood in Fort Worth.
“I’ll have these same conversations whether or not they are larger or smaller,” Igbokidi said. “Just being able to have these conversations is going to bring healing. It’s going to bring understanding and it’s going to allow the communities to become stronger.”
The federal government is trying to standardize data sharing so electronic health records (EHRs) across the country can all speak the same language. The Texas Medical Association is telling the government to keep working on it.
TMA submitted comments on the draft of version 3 of the United States Core Data for Interoperability (USCDI), which aims to establish data-sharing standards “for nationwide, interoperable health information exchange.” USCDI updates come from the Office of the National Coordinator for Health Information Technology (ONC), which released the version 3 draft in January. The first version of USCDI became part of certain EHR certification criteria.
In an April 27 letter to ONC, TMA offered several suggestions on how to improve the proposed new version, including:
Assign “applicable vocabulary standards” to any data elements added to the USCDI so there’s an established way to refer to those data across EHRs. “Adding nonstandard elements will result in an enormous amount of vendor and end-user work that will simply create nonstandard data that are difficult to transfer. It also will create an excessive amount of rework in the future once applicable vocabulary standards are set for these data elements,” TMA said in the letter.
Test EHR vendors and users to ensure a smooth transfer of data from previous USCDI versions 1 and 2. TMA told ONC it is hearing from physicians already frustrated “because of the manual manipulation of data received [from EHRs] that places additional burden on practice staff who are already stretched thin.” Information that a physician receives from a hospital, TMA said, “is not always in a human-readable format or is so limited as to be not useful or actionable.”
In fact, then-TMA President E. Linda Villarreal, MD, and Ogechika Alozie, MD, chair of TMA’s Committee on Health Information Technology, urged ONC to delay finalizing and requiring the new USCDI version “until EHR vendors prove their users are able to functionally use USCDI versions 1 and 2 and that all data elements” are streamlined.
“Patricia” has one main goal in life: to love and provide for her three young children. But when the single mother suffered from a painful umbilical hernia, it caused so much physical stress on her body that she was unable to work. And though she still trudged through family activities, the pain made her emotionally distant. Everything important to her was being compromised, and she worried about their future – especially that of her seven-year-old, who has special needs.
“The pain was bearable in the beginning, but as time went on it was getting worse, and my belly button was sticking out,” Patricia says. “I fortunately did not have to go to the ED, but I did resort to pain medication for relief.”
She knew continually taking pain medicine was not a good long-term option, so Patricia went to Mission Arlington for treatment, thinking she might have ovarian cysts. Instead, she found out about the hernia and that she would need surgery. In that moment, she was overwhelmed by fear.
“I did not have the money,” she says. “And who would take care of my kids? How would they be provided for? A lot of thoughts came racing through my mind.”
Then Patricia was connected to Project Access, and everything began to change. She realized she wouldn’t face the financial avalanche of paying for a surgery she couldn’t afford, and she was going to finally get help for the pain that was holding back every part of her life.
Now as Patricia heals from the hernia repair, she tries to put the impact into words.
“The surgery was done perfectly,” she says. “I don’t have any pain anymore, and when I have my menstrual cycle, it is normal. It is no longer heavy or overbearing. I can do anything now; I feel amazing!”
She thanks God for using the doctors and Project Access to provide much-needed care and prays that all who helped continue to be rewarded for their service. “I will always be grateful for everything Dr. Saad has done,” Patricia says. “I am so thankful for the support I received since day one and for guiding me through the process. I would not be where I am now without PATC.”
This article was originally published in the March/April 2022 issue of the Tarrant County Physician. You can read find the full magazine here.
Two roads diverged in a yellow wood, And sorry I could not travel both And be one traveler, long I stood And looked down one as far as I could To where it bent in the undergrowth;
We all had a choice. We graduated from medical school and then picked a residency along the way. We knew that this choice had to be lasting. That was a lot of pressure for those of us who think too deeply or gaze off too far toward the horizon. And yet, the decision was made, none of us grasping the fact that an even bigger decision lay ahead of us just around the bend, past the undergrowth.
Then took the other, as just as fair, And having perhaps the better claim, Because it was grassy and wanted wear; Though as for that the passing there Had worn them really about the same,
What did we do next? Some chose academics, though that was a minority. An even smaller minority chose private practice. And many chose to join the world of corporate medicine, working for hospitals or insurance conglomerates or large multispecialty groups. That may be three roads, not two, but you get the gist.
And both that morning equally lay In leaves no step had trodden black. Oh, I kept the first for another day! Yet knowing how way leads on to way, I doubted if I should ever come back.
At the time, all of these choices looked to be equal. It felt right, though, that I would start my own business, put out my shingle, a welcome mat of sorts, try my luck, and let the cards fall as they may. And fall they did. For 20 years, I have run a business, something I was never trained to do. I have built a successful practice (knock on wood), successful not because I’ve made a lot of money, something solo primary care physicians rarely do anymore, but because my staff and I have helped a lot of people live better, fuller lives. Above all else do no harm, but that really means do the best for your patients, their families, our friends, and all of us.
I shall be telling this with a sigh Somewhere ages and ages hence: Two roads diverged in a wood, and I— I took the one less traveled by, And that has made all the difference.
But now, it is so much easier to look back and ponder a new choice. With the advent of quality measures, ever-changing metrics where the finish line is constantly moving, with the dissolution of the fee-for-service system, it has become infinitely harder to run a small practice. To oversimplify, we don’t always know where or when revenue will come in, and the variability increases with the fact that we never know how much we will be paid for the work we do. And when my patients remind me that I’m not doing it for the money, I also remember that without the incoming stream of revenue, I would not have a practice that does so much good for my people, my friends, my patients. Perhaps as I continue to walk this chosen path, I will cross a stream or two, get tangled in the brush, maybe even trip, fall, and get back up again. No matter what, as all of us who are in small practices are apt to do, I continue forward, not knowing what lies ahead. Perhaps I will come to another place where two roads diverge in the woods, and I will have to choose again. For now, I bow to one of the Greats, and let Robert Frost have The Last Word.
This article was originally published in the May/June 2022 issue of the Tarrant County Physician.
Photo credit: Texas Medical Association
On April 30, 2022, longtime TCMS member and past president Dr. Gary Floyd was installed as TMA’s 2022/2023 president. A pediatrician who has practiced in Tarrant County for over 40 years, Dr. Floyd sat down with the Tarrant County Physician to talk about everything the led him to this point, and what he anticipates for this next year as he takes the helm of one of the largest medical associations in the country.
Q So Dr. Floyd, what would you say, in your opinion, is the best thing about being a doctor?
A You know, I think the best part or the most amazing part to me is that people, and in my case families, trust you enough to take care of their children. And for adult docs, those patients trust them enough to take care of them. I have always just stood in awe of that. The second part for me has been the collegiality, and that has come both in the workplace and through organized medicine. I have over the years made many acquaintances, many friends, and that’s just not replaceable.
Q Speaking of the physicians you’ve worked with, how do you think organized medicine – TMA specifically or any of the multiple organizations you’ve worked with over the years – impacts both physicians and patients?
A I think organized medicine gives us a collective voice for the issues that plague all of us. We can usually come to common consensus, and it gives us a large body of people, a large number of physicians, who will speak out for our issues. And instead of just one person crying in the wilderness alone, you go representing fifty-six thousand members of TMA. People start listening in.
Q That makes a lot of sense. So, on advocacy: what do you think are some of the most important ways that advocacy has impacted the practice of medicine? I know there’s a pretty long laundry list.
A There’s a long list, yes. I think for Texas physicians one of our biggest achievements or wins was our liability reform that occurred back in 2003, almost 20 years ago. Thanks to work with the public and literally grassroots in the office in talking to patients, this went before the public in a proposition for a constitutional amendment and passed. So hats off, not only to the physicians who worked so hard on that but to the public who understood the need to bring in more physicians to Texas.
I think you’d also have to hallmark [that TMA] sued CMS and won in the district court in Tyler and now we’re waiting for their appeal. This had to do with the No Surprise Billing act. Congress got it right in their wording and had a very fair independent dispute resolution process. But in writing, CMS’s rules initially came out very much in favor of insurance companies and detrimental to physicians. So that’s why Texas sued and won. It’ll be interesting to see how this will pan out, and whether the federal government will appeal to a higher court. But we’re ready for that battle. It’s an expensive battle, but it’s well worth fighting for physicians and for patients.
Q You’ve talked about some issues that are clearly important to you. Focusing on your leadership roles: a lot of physicians are involved in organized medicine but only so many choose to actually get involved on the leadership level, which allows you to really participate in creating change. What inspired you to do so?
A I think every leadership position I’ve ever run for or been elected to, it’s been because others have asked me to do it, so I think it’s been because of the relationships that have been built with colleagues as we went through our normal course of work. Showing up to those meetings and participating in committees. And with respect to TMA, not only committees but councils; apparently people agreed with some of the things that were important to me and with the way that I could express that, and those were the folks that asked me to serve in various positions with TMA. And my wife says it’s because I can’t put my hand down and haven’t learned how to say “no!”
Q Looking back at some of your leadership roles between TCMS, TMA, AMA, and the different organizations you’ve been with, what have been some of the highlights along the way?
A I’ve had the incredible privilege to serve as president of Tarrant County Medical Society, now president-elect for the TMA. I’ve been very honored to serve as president for Texas Pediatric Society and president of the Texas chapter of the American Academy of Pediatrics. One of my most fun jobs was when I got to chair the TMA Council on Legislation. That was really a fun time – there was a lot of interaction at the capital, and I’m looking forward to that as president next year since it’ll be a legislative year starting in January.
But perhaps one of the most challenging positions was serving as chair of our TMA Board of Trustees during the pandemic when we had to become an emergency disaster board. Thanks to the great teamwork by all members of our Board, we got through it and managed to take care of the TMA business that needed handling.
Q Going back to the legislative session, what are some of your overarching goals for that? And what are some of the things you hope to accomplish during your presidency?
A My agenda is mainly just serving my fellow physicians in the best way I can. You know, I think we’ve really taken it on the chin with COVID. For two years there have been challenges from appropriate equipment shortages to a lot of garbage on the internet that has been very misleading. So my main goal for this year is for us as physicians to reclaim trust, to try to unify better, to try to communicate better, and try to find the common issues that we need to stress and push that really impact our patients. Also, to protect the autonomy of the patient-physician relationship however we can so physicians can address issues comfortably without either [patients or physicians] fearing interference from any of those other entities, be it government, be it insurance, be it hospital – whatever.
Q That concern is definitely a top issue. So what would you tell someone who is right at the beginning of their career, or the beginning of their involvement with organized medicine?
A For any physician just starting it’s really important for them to know who they are, so they have to have a support base. And for me that starts with faith, with my faith in the Lord. For them it may be something else, I don’t know, but I think that has really helped ground me. The other part of that is my family; they keep you grounded, and they keep it real. And then joining in with colleagues. Being not just a participant or a member but being and getting involved in organized medicine.
There’s a lot to be done. We have a lot of committees and councils that are doing excellent work and it’s finding what’s important to you and making the time. You literally have to make the time to get involved. You sacrifice some family time and time working in your practice. So you have to be aware of that; you have to plan. But I just can’t encourage people enough, to know how rewarding and how worthwhile it is to make that time to join with your other colleagues and be involved in organized medicine and join the leadership team.
Q So looking at this next year, it’s a very exciting time for you. You’ve had a great career; you got to help a lot of people in both practice and in organized medicine, but now you’re starting something new. Do you have anything you’d like the physicians of Tarrant County to keep in mind this next year?
A One thing I would say, not only to the Tarrant County physicians but those throughout the state, is to stick to issues. State opinions about issues, but insulting public officials is never going to get us anywhere, not even into compromised territory. Call me, call [TCMS CEO] Brian Swift, get it off your chest. But don’t put it out on social media; it rarely achieves anything.
For the folks in Tarrant County, I know practice and family and faith life are demanding, but I am an example that you can do organized medicine with all of that. I would encourage you to show up. Just come. The biggest part of getting involved is showing up. We are always looking for people to serve on committees and councils. I didn’t do anything special; I don’t have any special knowledge. The experiences I’ve gained are because I’ve shown up. It’s important to be involved now, because the practice of medicine is being challenged in many ways, and it is your chance to make a difference for your practice and your patients. So show up; you’ll be glad you did.
In our next issue, you will again hear from Dr. Floyd as he reports on his experience as TMA president and highlights TMA’s top priorities.
When Trey Moore, MD, started his career as a urologist in Fort Worth 26 years ago, he worked in a busy emergency department and his own private practice. In both settings, many of his patients weren’t covered by insurance and could only access stopgap care. At the same time, he was surprised by the dearth of opportunities for physicians like him to give back to their community by offering their services pro bono.
So, in 2011 he jumped at the chance to join Project Access Tarrant County, a then-nascent initiative of the Tarrant County Medical Society (CMS) that connects low-income, uninsured residents to specialty and surgical services provided by a network of volunteer physicians and facilities. Since its start, Project Access has served more than 1,700 patients and provided more than $14.5 million in donated health care.
Dr. Moore especially likes the program’s focus on surgical care, which is unique in the world of health care safety-net programs. Given his specialty, many of his neediest patients – such as those suffering from large kidney stones that cause recurring, and sometimes disabling, infections – require surgery to recover fully.
“Every [pro bono service] makes a difference, whatever we do, but [Project Access is] particularly helpful because so many of these patients – until they have a surgical resolution – are stuck in a vicious cycle of not being able to go back to work and cycling in and out of emergency rooms,” he said. “It’s a big stress on the patients and their families, and it’s a big stress on the system.”
But relieving that stress would not be possible without ongoing financial support.
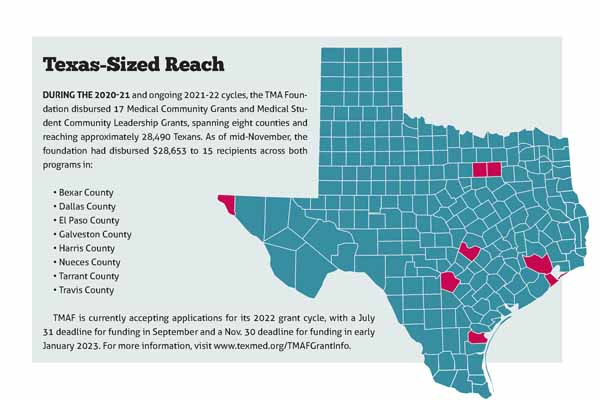
Project Access is one of several long-standing recipients of the Texas Medical Association Foundation’s Medical Community Grant program, which accepts applications from county medical societies and alliance chapters for up to $7,500 in matching funds to support unique community health improvement initiatives. The separate Medical Student Community Leadership Grants program accepts applications from TMA medical student chapters for up to $3,000 thanks to a fund established by Houston pathologist Roberto J. Bayardo, MD.
For more than two decades, TMAF’s grant programs have helped the Family of Medicine tackle the state’s most pressing health care concerns at the local level. Many grantees, including Project Access, have received funding over successive years, which allows for continuous programming. Physicians like Dr. Moore say this is especially important in Texas, which has the highest rate of uninsured residents in the nation.
Not only do the grant programs connect patients to life-changing care but also they honor TMA’s mission to stand up for Texas physicians by providing them with resources to create solutions to local health challenges and by reinforcing physicians’ trusted leadership in the community, says TMA Foundation Executive Director Lisa Stark Walsh.
“Our goal is to remove the obstacle of resources for members to do what they feel is necessary in their communities,” she said. “Medical Community Grants give physicians an opportunity to chip away at long-standing, intractable problems over the long term and to demonstrate their advocacy for the health of all Texans.”
Originally founded in 1966 as the Texas Medical Education and Research Foundation, TMAF is a separate, nonprofit entity that serves as the philanthropic arm of TMA. Since 1998, the Medical Community Grant and Medical Student Community Leadership Grants programs have disbursed $891,931 across more than 200 such grants to support myriad community health improvement programs all over Texas, ranging from vaccine clinics and border health services to breast cancer screenings and kids’ bicycle helmet giveaway events.
Houston neonatologist and TMAF Board President Michael E. Speer, MD, is passionate about growing the foundation’s endowment so it can offer even more grants that support Texas physicians and their patients. “If you look at the most successful colleges and charities, the best ones spend very little on themselves and most of their endowment on supporting the organization,” he said.
This growth mindset has paid off. In recent years, TMAF has fielded increased demand for the grant programs from county medical societies, alliance chapters, and medical student chapters. As a result, the upcoming application cycle will include a new focus area of physician health and wellness. This expansion stems from the success of a recent TMAF initiative, Caring for Physician Healers: Mental Health and Wellness Resources During COVID-19 Fund, which helped seven county medical societies launch or extend physician health and wellness initiatives during the ongoing pandemic. (See “Self-Investment: Physician Wellness Programs Bolster a Beleaguered Workforce,” November 2021 Texas Medicine, pages 22-25, http://www.texmed.org/Self-Investment.)
By harnessing the expertise of medicine to help address a community health problem, the TMAF grant programs complement the work of the association and represent the best of organized medicine, says TMA President-Elect and TMAF board member Gary Floyd, MD.
“Anyone in practice will find things that need to be changed,” he said. “When you’re alone or in a small group, you’re just a small voice yelling into the wind with very little result. When you join into organized medicine, particularly with TMA, you have [more than] 55,000 voices, and people tend to start listening.”
Physician-driven results Tarrant County Medical Society received its eighth TMAF Medical Community Grant in support of Project Access in 2021. The program’s organizers say it is a prime example of what physicians can accomplish working together to solve an entrenched community health problem. Tarrant CMS was inspired by the Dallas County Medical Society’s now defunct Project Access initiative, which focused on primary care. Given Tarrant County’s robust network of free and income-based primary care clinics, Tarrant CMS decided to gear its own Project Access initiative toward specialty and surgical care since that’s where the need was most acute.
Tarrant CMS Executive Vice President and CEO Brian Swift says Project Access runs on a shoestring budget that belies its impact. Patients are largely members of the working poor, and many are undocumented immigrants. They don’t qualify for Medicaid but typically don’t earn enough to afford private insurance, leaving them without coverage and beholden to emergency departments for symptom management. Without care that addresses the root cause of their medical problems, however, they are often robbed of their livelihoods – and sometimes their lives.
By providing specialty and surgical care to eligible Tarrant County residents, the initiative not only helps patients resume healthy lives but also saves area hospitals tens of thousands of dollars in emergency department costs. “These patients don’t have access anywhere else,” said Stuart Pickell, MD, Project Access’ medical director and an internist-pediatrician in Fort Worth.
Although physician volunteers provide specialty and surgical care, Project Access still requires funding to fulfill its mission. “Free isn’t free,” Mr. Swift said.
As with previous awards, the county medical society used the TMAF funds to offset the costs of its annual patient database subscription. “Data management does not come cheaply, so we really depend on that [funding] to be able to manage our Project Access database,” Mr. Swift said.
The grant-funded database – which Dr. Pickell describes as “essential” – allows staff to determine patients’ eligibility, which helps ensure Project Access is distributing its limited resources as judiciously as possible, and to track their care, including the donated value of medical services and administrative costs. In this way, the grant helps Project Access obtain more funding by quantifying its positive impact and cost savings.
Armed with the database, staff can focus on serving patients – and the broader community. Typical cases include a woman with cervical cancer who would have died without surgery, leaving her young children orphans; a construction worker with a hernia that kept him out of work; and a patient with osteoarthritis that had nearly disabled her until surgery allowed her to resume a productive life.
The Project Access model not only unburdens its patients and their loved ones from medical crises but also often allows them to return to work. This can be transformative, Dr. Pickell says, because a job offers the possibility of long-term health care access through employer health insurance.
After a decade of success, staff are now working on growing the program. With more than 500 volunteer physicians across numerous specialties, including ancillary care, their attention is focused on the limiting factor of operating room space and other facility needs. By renting such space, rather than relying on the whims of donors, Project Access can increase its patient volume.
Physicians would welcome such a change. “It’s such a gracious group of people,” Dr. Moore said. “They’re so grateful to get help. In a selfish way, it’s a great group to treat.”
Project Access also is keen to expand, both to meet the community need and to highlight the work physicians do every day to serve their patients. It’s supported in this endeavor by TMAF’s Medical Community Grant program, which allows physicians to spearhead solutions to the problems they’re facing on the ground.
“That’s why it’s so important for the foundation to continue doing what it does,” Mr. Swift said.
An engine for innovation Another repeat recipient, in this case of the TMAF Medical Student Community Leadership Grants program, the annual HOPE Health Fair in Galveston tackles a community health challenge while also providing medical students with the opportunity to fine-tune solutions over the long term.
The University of Texas Medical Branch (UTMB) TMA Medical Student Section chapter hosted its fifth annual event in November thanks, in part, to its fourth annual TMAF grant award. The fair connects approximately 250 uninsured Galveston residents – around a quarter of whom are homeless – to vaccinations, health care screenings, meals, and educational resources through the St. Vincent’s Student Clinic at UTMB. It also serves as a critical outreach opportunity in Galveston County, where 17.4 percent of residents under age 65 lack health insurance, according to the U.S. Census Bureau.
“We’re just catching ships in the night, people who frequently never have access to health care,” said John W. Davis, one of the event’s organizers and a third-year medical student at UTMB who also is pursuing a PhD.
The HOPE Health Fair received a $3,000 Medical Student Community Leadership Grant from TMAF in 2021, which covered about 40 percent of the overall cost. Without it, organizers would not have been able to host the event. “It’s very helpful for us to get this grant each year,” said Jenna Reisler, a third-year medical student at UTMB and an event organizer.
In addition to providing critical funding, the grant also has spurred innovation. Because the organizers are repeat recipients of the grant program, they take pains to improve the event each year. In 2021 they used the award to offer rapid COVID-19 testing and screenings for sexually transmitted infections, including HIV and hepatitis C.
By offering screenings, the organizers not only help attendees detect any debilitating illnesses they might have contracted but also prompt them to return to the student clinic to get their results and receive treatment. Once attendees have made the jump from the health fair to the student clinic, they can receive treatment for underlying health problems, such as diabetes and hypertension, and start to build patient-physician relationships.
In this way, the health fair functions as a kind of benevolent Trojan horse, linking Galveston’s most vulnerable residents to health care for years to come. “It’s a way to show people that we care about them,” Mr. Davis said.
Global reach Located in a top U.S. county for refugee resettlement, the Baylor College of Medicine (BCM) TMA Medical Student Section chapter and the Houston nonprofit Alliance for Multicultural Community Services have used the TMAF Medical Student Community Leadership Grants program to host the BCM-Alliance Refugee Health Fair. The annual event helps refugees navigate the local health care system – and provides medical students a glimpse at global health in action.
Like the HOPE Health Fair, the BCM-Alliance Refugee Health Fair aims to serve as a conduit for attendees to long-term health care access. At an upcoming event scheduled for this spring, student volunteers will distribute hygiene kits – including soap, hand sanitizer, masks, and health care resources in multiple languages – via a COVID-19-safe drive-thru. Attendees also will receive basic preventive health screenings and flu vaccines from local free and income-based clinics.
Although refugees can access Medicaid for up to eight months upon their arrival in the U.S., they are expected to secure private insurance afterward. This is a complicated process that can quickly fall to the bottom of a refugee’s to-do list, overtaken by tasks such as learning a foreign language, securing a job, and familiarizing oneself with the local public transit system. But the BCM-Alliance Refugee Health Fair aims to smooth attendees’ search for health care by introducing them to the Alliance and area clinics.
“Ultimately, even if these patients don’t stay on with these clinics, they at least have a starting-off point to return to if they develop a medical issue in the future,” said Avery Haugen, a fourth-year medical student at Baylor and one of the event’s organizers. “It really alleviates a lot of the stress of those first steps.”
The Baylor TMA student chapter will use its latest TMAF grant – its fifth – to print promotional flyers, purchase hygiene kit supplies, and furnish volunteers with personal protective equipment. The grant, which accounts for nearly all of the event’s budget, is critical to its success.
“This event is really not possible without the help from the TMA Foundation,” said Chris Wong, a fourth-year medical student at BCM and another event organizer.
In addition to educating refugee attendees about the local health care system, the event also serves as a critical learning experience for the medical students involved. Both Ms. Haugen and Mr. Wong are interested in global health, which is partly what prompted them to get involved with the fair.
“The event was really my first exposure to the idea of refugee health [and] the very specific health disparities that immigrants face, especially in our very complicated health system,” Mr. Wong said.
Similarly, Ms. Haugen sees the event as a unique opportunity to learn more about global health while studying medicine in Houston – and largely prohibited from international travel by the ongoing pandemic.
“For us, the refugee health fair is a really unique example of a way to promote global health on a local scale,” she said.
Find Texas Medical Association’s original press release here.
On Saturday, April 30, 2022, the Texas Medical Association (TMA) installed Gary W. Floyd, MD, a Keller pediatrician, as its 157th president. TMA’s House of Delegates policymaking body installed Dr. Floyd during TexMed, the association’s annual conference, in Houston this year. TMA elected him president-elect in May 2021.
“It’s an incredible privilege and responsibility – and very humbling – for the members of our TMA to entrust me to lead our great organization,” Dr. Floyd said.
Three tenets guide him: his work, faith, and family. He said the three principles have formed the internal value system by which he lives and works, serving as guardrails along his path from medical school to TMA president.
Dr. Floyd addressing the members of the Texas Medical Association as their newly-installed president.
Dr. Floyd is the fourth president to serve America’s largest state medical society during the ongoing COVID-19 pandemic. During his one-year presidency, he hopes to repair the mistrust of the medical profession that has grown as doctors and health care workers have battled COVID. He said to accomplish that, organized medicine should present a united front in the face of misinformation, while remaining professional and collegial.
“One of the biggest things we have to focus on … is finding areas of commonality,” Dr. Floyd said.
He explained those commonalities include “protecting the sanctity of the patient-physician relationship; allowing physicians to practice medicine without … interference from insurance or other payers or the government; protecting our patients as they seek assistance for delicate issues; and protecting our physicians as they try to render care to the best of their abilities.”
Dr. Floyd has been involved in TMA throughout his 43-year medical career. He chaired the TMA Board of Trustees, the association’s governing body, in 2020-21, having served seven years on the board.
He also chaired the TMA Council on Legislation and served on the association’s Council on Constitution and Bylaws, and the Select Committee on Medicaid, CHIP, and the Uninsured. Dr. Floyd also was a district chair of TEXPAC, TMA’s political action committee.
In addition to his TMA involvement, he previously served as president of the Texas Pediatric Society and the Tarrant County Medical Society, and he was active in the American College of Physician Executives and the Society for Pediatric Emergency Medicine. He is a fellow and board member of the American Academy of Pediatrics.
After the pandemic hit, Dr. Floyd began seeing fewer patients although he continues to be involved in medical management and organized medicine. His passion for medicine makes him a strong advocate for patients and physicians. His recipe for successful advocacy involves teamwork. One example, he said, was the agreed-to bill he helped TMA broker with advanced practice nurses and physician assistants in 2013. The Texas Legislature passed the landmark compromise, which led to an improved model for a team-based approach to health care, with physicians leading the team.
Dr. Floyd believes successful advocacy does not happen overnight; it depends on unwavering, grassroots commitment. “It’s not that you have special abilities,” he said, “it’s just that you keep showing up.”
Dr. Floyd is board certified by the American Board of Pediatrics. He has practiced in various settings in Texas and Oklahoma including general pediatrics, academic pediatrics, and pediatric emergency and urgent care. He was the medical director for pediatric emergency services at Cook Children’s Medical Center for 15 years. Dr. Floyd later became John Peter Smith Health Network’s chief medical officer and executive vice president of medical affairs, and then executive vice president of government and alumni affairs.
A graduate of The University of Texas Medical Branch School of Medicine at Galveston, Dr. Floyd completed his pediatric residency at Children’s Hospital of Oklahoma, University of Oklahoma Health Science Center. He pursued his undergraduate studies at The University of Texas at Austin.
Dr. Floyd has been married 47 years to Karen Floyd, whom he met when they were in high school. She introduced him to Christianity – a faith that he said kept him calm when he found himself in chaotic pediatric emergency departments and intensive care units, with patients sometimes on the brink of death.
The couple has two married daughters, Holly Peterson, married to Ben Peterson; and Neely Pedersen, married to Craig Pedersen, DO; and three grandsons.
This article was originally published in the March/April 2022 issue of the Tarrant County Physician. You can read find the full magazine here.
In response to soaring overdose deaths across the U.S. during the pandemic, the American Medical Association (AMA) Advocacy Resource Center published a brief on Nov. 21, 2021, cataloging increased overdose deaths state-by-state. They decried decreased access to “evidence-based care for substance use disorder, chronic pain, and harm reduction services.”1
The AMA also sent a letter to the U.S. Centers for Disease Control and Prevention urging requirements for health insurers to eliminate barriers to opioid treatment for patients who would benefit from these therapies (think prior authorizations for prescriptions and faxed referrals for specialists). The letter also supported the Biden Administration’s 2022 National Drug Control Strategy, which highlights increased production of medications for substance use disorders, harm reduction strategies (including needle and syringe exchange programs), access to naloxone without prescription, and elimination of health insurer obstacles which prevent persons with chronic pain from accessing pain management.3
In addition, a letter from AMA’s Dr. James Madara, MD, to Regina M. LaBelle, the acting director of the Office of National Drug Control Policy, on July 9, 2021, stated that healthcare inequities and social determinants of health fueling the overdose epidemic and disproportionately affecting the “marginalized and minoritized” must be addressed.2
The National Vital Statistics System recently released its “Provisional Drug Overdose Death Counts” for 2021 for the fifty states and the District of Columbia.4 The total overdoses will likely be revised upwards as case compilations for 2021 are completed and reports verified, but the provisional death toll is staggering. Over the 12-month period which ended in June 2021, overdose deaths rose from 47,523 to 98,022, and in Tarrant County, our overdose deaths mirror the national trend with 350 overdose deaths for the 12-month period ending March 2021, compared with 185 overdose deaths for the 12-month period ending January 2021. (Tarrant County data are not yet available for April – December 2021 on the NVSS dashboard.)
Overdose deaths provide one measure of the toll of COVID-19 in the U.S. and expose need for redress of healthcare inequities, access to medication for opiate use disorders, substance use disorder treatment, mental healthcare access, and access to pain management. Another way the impact of COVID-19 is being assessed is through peer-reviewed publications exploring the hidden costs and benefits of conventional in-person (commuter) work versus work from home.
“Over the 12-month period which ended in June 2021, overdose deaths rose from 47,523 to 98,022, and in Tarrant County, our overdose deaths mirror the national trend with 350 overdose deaths for the 12-month period ending March 2021, compared with 185 overdose deaths for the 12-month period ending January 2021.”
The results of such studies are uneven and the responses necessarily somewhat subjective when subjects are questioned regarding their feelings about in-person versus telework; in general, workers viewed telework more favorably when they volunteered for it and when their schedules included a combination of both in-person and telework. When mandatory, some teleworkers experienced increased “work-family conflict” as the lines between work and domestic life blurred during telework. Teleworkers and conventional in-person workers reported variable effects on depression, exhaustion, fatigue, and energy level.5
Using data from the American Time Use Survey, authors asked workers to record in a diary where they worked (whether they commuted or not) and noted that male teleworkers in this study reported lower pain, stress, and tiredness levels, but that there was no difference in these measures among female commuters versus non-commuters.6
In another study based on the American Time Use Survey, the designers compared pain in working-at-home versus conventional workers and found no difference in pain reporting between the two groups. However, working-at-home fathers reported increased stress and working-at-home mothers reported decreased happiness.7
COVID-19 is, at the very least, an engine powering academic inquiry, which may have unexpected future benefits for the way healthcare is delivered and work is done. In the meantime, we must continue the important work of educating, advocating, and caring for our communities.
References 1. AMA Advocacy Resource Center: Issue brief: Nation’s drug-related overdose and death epidemic continues to worsen, Updated 11/12/2021
2. AMA letter to Regina M. LaBelle, Acting Director of Office of National Drug Control Policy, 7/9/2021
3. AMA letter to the U.S. Centers for Disease Control and Prevention, June 2020
5. Oakman J et al. A rapid review of mental and physical health effects of working at home: how do we optimize health? BMC Public Health (2020) 20:1825
6. Song Y, Gao J. Does telework stress employees out?A study on working at home and subjective well-being for wage/salary workers J Happiness Stud 2019;21(7):2648-68
7. Gimenez-Nadal JI, Molina JA, Velilla J. Work time and well-being for workers at home: evidence from the American Time Use Survey. Int J Manpow 2020; 41(2): 184-206
Originally published by TCU School of Medicine on April 19, 2022. You can read the original article here.
TCU School of Medicine welcomed experts from Olympus, global leaders in the development of medical devices, onto their campus in early February to give medical students an immersive and hands-on experience using the latest laparoscopic surgery equipment.
Jim Cox, M.D., an assistant professor at TCU School of Medicine, helped organize the event with the help of the Gastrointestinal and Hepatology Student Interest Group (SIG).
“When I was in private practice I worked extensively with Olympus and I reached out to a former colleague and asked could you provide this training session for the students,” Dr. Cox said. “The thing with Gastroenterology is that much of what we do is colonoscopy or upper endoscopy. We have first, second- and third-year medical students here just to give them the opportunity to see if they’re interested in Gastroenterology.”
Before immersing themselves into the technology, about two dozen medical students joined Dr. Cox for a brief presentation in the simulation lab. He gave a brief overview of typical things the students might see during residency.
“Let’s say an ulcer or a polyp or colon cancer and how are we going to treat those things,” said Dr. Cox. “Are we going to remove them? Are we going to remove an inanimate object from the esophagus that someone inadvertently swallowed? We’re talking about both urgent and non-urgent procedures that gastroenterologists encounter every single day.”
The medical schools’ simulation lab had laparoscopy training monitors and tools provided by Ethicon. The training monitors allow the students to see simulated examples of a laparoscopy, which are small scars on the abdomen. Students can use the monitors attached to the machine to practice suturing and knot tying techniques that require basic hand-and-eye coordination.
“This requires more than just being able to coordinate your hands,” said Sujata Ojha, a third-year medical student and co-president of the Gastroenterology and Hepatology Student Interest Group (SIG) at TCU School of Medicine. “There’s visual spatial movement and being able to know where you are in space and being able to maneuver without impacting the patients’ internal organs.”
Dr. Cox added that most of today’s gastrointestinal surgeries are done using a laparoscope, which makes this training much more beneficial for medical students.
“Most gallbladder, appendix and other intraabdominal organ removals are done using a laparoscope,” Dr. Cox said. “They leave very tiny scars which may actually go away in a few years as opposed to having the patient needing a big scar that could possibly stay for a lifetime.”
Gastroenterologists are advancing more and more into the use of laparoscopic procedures. A recent 5-year patient study presented at the 2022 International Gastric Cancer Congress in March showed laparoscopy surgery compared with an open gastrectomy surgery was found to produce better overall survival outcomes for patients, according to the Cancer Network.
Mallory Thompson, a third-year medical student and co-president of the GI and Hepatology SIG, was excited about the demonstrations at the medical school.
“Medical students aren’t exposed to these kinds of medical procedures during their clinical rotations this is more for medical resident training,” Thompson said. “It’s exciting that our medical school faculty like Dr. Cox and our student interest group are setting up these kinds of opportunities for us.”
This article was originally published in the March/April 2022 issue of the Tarrant County Physician. You can read find the full magazine here.
“I’ve done my research.”
These can be some of the most dreaded words to hear as a physician from our patients and their families. We can spend seven-plus years in medical school, residency, and sometimes fellowship, studying our field before we embark on our journey to practice medicine. We also hone our craft through continued learning throughout our careers. Yet, we are often confronted with the above phrase. Since when did Dr. Google become such an expert that it can supersede our years of training and practice?
This became ever more apparent as the COVID-19 pandemic started over two years ago. (Yes, we have crossed over the two-year mark and are still counting). With a lack of information and understanding of this novel virus as well as increased access to information on the internet, we in science and medicine saw people seeking out answers from all the resources they had access to. This unfortunately led to propagation of numerous pieces of misinformation, distortions, and half-truths. Add to this the politicization of our nation and the polarization regarding best measures on how to handle the COVID-19 pandemic, and unfortunately, we in science and medicine are left as the ones not to be trusted.
As a women’s health physician, I am confronted with this on an almost daily basis. While the internet can be a valuable resource of information, it can also be a not so valuable resource of misinformation, lies, and myths. Misinformation was commonly passed along in relation to women’s reproductive health even before the advent of the internet. Unfortunately, nowadays it has a much wider reach with the “expertise” of Dr. Google to further spread these untruths.
What are we to do in this constant back and forth of the internet versus the doctor?
For me, I try to meet my patients and their families where they are. I work with them to better understand where they are coming from as well as who or what their source of information is. I cannot undo the vastness that is the internet and Dr. Google, but I can work to build a relationship with my patients and their families to come to shared decision making to provide the best care for them.
“For me, I try to meet my patients and their families where they are. I work with them to better understand where they are coming from as well as who or what their source of information is. I cannot undue the vastness that is the internet and Dr. Google, but I can work to build a relationship with my patients and their families to come to shared decision making to provide the best care for them. “
While this is helpful in individual encounters of patient care, I also feel that it is important for us as physicians to be out in the public arena as well. Because of this, I never turn down an opportunity to speak when asked, and I am always happy to provide my expertise for those in the media. As physicians, we have a duty to educate. This is a responsibility not only to the individual patients we take care of, but also to the public. By offering education that is based in science and grounded in our years of continued study and experience, we can work to counteract the vast amount of distorted information that is out there. I, for one, will continue in my efforts to dispel myth and spread truth.