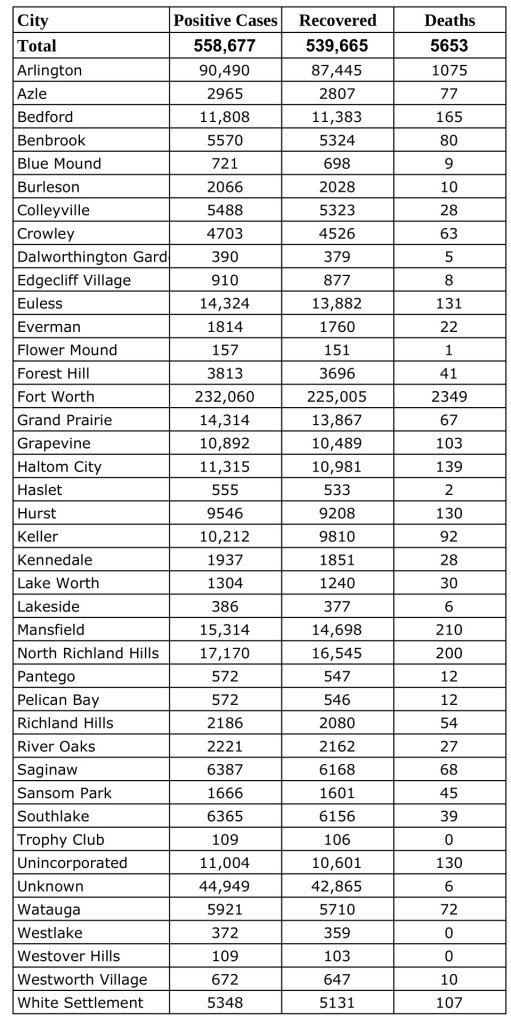
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County updated Wednesday, March 2, 2o22.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.
The AMA-MSS Region 3 includes medical schools in Arkansas, Kansas, Louisiana, Mississippi, Oklahoma and Texas.
“My job is to learn about what different health care policies are being passed in these different states,” Singh said. “And spread that news and raise awareness among medical students because as we all know these policies impact everyone from students to physicians and patients.”
Singh will oversee the Region 3 advocacy committee and lead advocacy initiatives to engage region chapters.
He will also work with the Advocacy Subcommittee of the Committee on Legislation and Advocacy (COLA) to help our region engage with events like National Advocacy Week (NAW) and the Medical Student Advocacy Conference (MAC). He will also support the Membership Chair and Secretary in reaching out to local chapters to highlight advocacy endeavors and provide advocacy updates in AMA-MSS Region 3 monthly newsletters.
“Policy writing is very niche and not every physician has to do that but the way this connects with the medical school is how they teach us to be an advocate for your patients,” Singh said. “And growing that idea on a larger scale its advocating for your population. Not only talking to physicians you’re talking to legislative members, congress members and kind of impact a larger audience that’s a really great opportunity as future physicians.”
The Medical Student Section (MSS) aims to be a voice for medical students’ across the AMA to help improve medical education and advocating for the future of medicine.
Statement by Diana L. Fite, MD, Texas Medical Association (TMA) immediate past president, in response to the U.S. District Court for the Eastern District of Texas’ ruling on TMA’s motion for summary judgment in its lawsuit opposing federal regulatory agencies’ unlawful approach to dispute resolution under the No Surprises Act.
“TMA is pleased that the court granted its motion for summary judgment in its lawsuit challenging the federal agencies’ unlawful approach to resolving disputes under the No Surprises Act. This decision is a major victory for patients and physicians. It also is a reminder that federal agencies must adopt regulations in accordance with the law.
“This decision is an important step toward restoring the fair and balanced process that Congress enacted to resolve disputes between health insurers and physicians over appropriate out-of-network payment rates. The decision will promote patient access to quality care when they need it most and will guard against health insurer business practices that give patients fewer choices of affordable in-network physicians and threaten the sustainability of physician practices.”
TMA is the largest state medical society in the nation, representing more than 56,000 physician and medical student members. It is located in Austin and has 110 component county medical societies around the state. TMA’s key objective since 1853 is to improve the health of all Texans.
This piece was originally published in the January/February 2022 issue of the Tarrant County Physician. You can read find the full magazine here.
Deciding to become a doctor meant comparing myself to numbers my whole academic career. In high school, I put my self-worth in my class rank and SAT score. In college, my sense of self relied heavily on my GPA, MCAT score, and volunteer hours. Getting anything less than an A (which happened more often than I would like to admit) sent me into a spiral of anxiety. I found myself scouring through online forums such as Reddit and Student Doctor Network to see where I stacked up to my peers. I would compare my GPA and MCAT score to the acceptance data provided by schools to determine if I was truly worthy of applying to that school. The uncertainty and stress of being a pre-medical student caused me to value numbers over relationships, but I told myself that one day, it would be worth it.
The sad reality was that in an effort to succeed, I had isolated myself emotionally and physically. These numbers I was chasing had come at a cost – I had become so single-minded that I had conditioned myself to study alone. I found class, study groups, and review sessions pointless because, in my mind, I was counting the hours down to when I could be alone at my desk, studying how I thought was best.
I started medical school in 2020 during the height of the pandemic. I had a positive mindset going in, but the first semester was one of the hardest times of my medical career. The forced social isolation stripped me of any sense of drive. I started missing class, my mental health declined, and my grades reflected my inner turmoil. The propensity for self-imposed seclusion that I had developed came back with a vengeance and worsened my cycle of apathy and misery. I struggled silently.
Things did not get much better during my second semester, so when I saw a classmate post about forming a study group called “Booked Up Together” over Zoom, I figured it was at least worth trying. As dramatic as this sounds, there was a little voice in my head telling me that I needed to admit that my way was not working, and I had to try something different. Let me tell you – I am so glad that I listened to that side of myself. Time that would have normally been spent alone in my room was now filled with friends quizzing each other and breaking down lecture material in a way that was easier to understand. Joining Booked Up Together was hands-down the best decision I have made since starting medical school. I started going to class, my mental health improved, and my grades got better. I became friends with warm and genuine people who helped me see the importance of not going through school alone. Study group became a safe space – I knew even on my bad days, there were people who understood and related to the pressure and stress.
Healthcare is multifaceted. As physicians, we will work together with different specialties and healthcare workers to ensure our patients receive the best care possible. While we are told that medicine is collaborative, the journey through medicine often feels solitary. I suppose it seems obvious now, but it is vital to protect our humanity while going through medical education not only for ourselves but for our future patients. For me, studying with my classmates reminded me that medicine at its root is a collective field, and while it is easy to get swayed by numbers and resume building, it is also important to remember why we decided to become physicians in the first place. What worked for me might not necessarily work for someone else, but I believe finding an avenue to collaborate is a beneficial way to stay connected with that part of yourself. Medical school is hard but going about it alone is even harder.
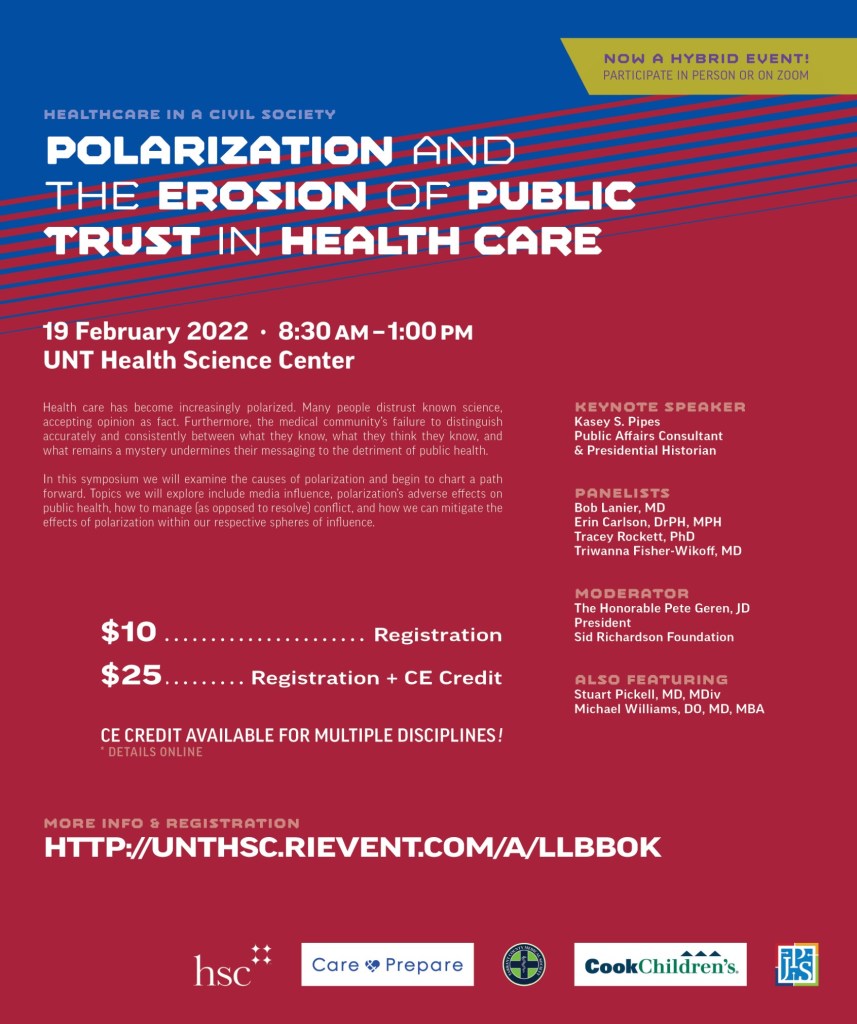
Tomorrow, Feb. 19, 2022, the Tarrant County Academy of Medicine Ethics Consortium, in partnership with the Tarrant County Medical Society, will host their annual Healthcare in a Civil Society symposium. This year’s program, “Polarization and the Erosion of Public Trust in Healthcare,” is an interactive event that takes an in-depth look at the impact of political polarization on healthcare.
“Our nation is beset by radical polarization,” says Stuart Pickell, MD, TCMS president-elect and chair of the consortium. “Historically, healthcare policy has been one topic on which we have been able to find common ground. What happened to transform it from something broadly bipartisan to incredibly divisive? This event will explore how we got to this point and begin to chart a path forward.”
The goal is to engage leaders of all perspectives in a civil conversation centered on the healthcare issues that are important to the Tarrant County community without the rhetoric that often undermines these conversations. This hybrid in-person/Zoom event will be held at the UNT Health Science Center from 8:30am to 1:00pm and provides continuing education credit for multiple healthcare disciplines.
While this symposium highlights discourse between community leaders, anyone who is interested in this critical topic is welcomed and encouraged to join the conversation. Those who are interested in participating can register here.
The event includes a breakout session allowing participants to explore the issues more deeply in small groups. A number of topics will be addressed, including:
How the media can influence public opinion and promote polarization
The impact of polarization on the public trust and public health
How polarization creates conflict (e.g., in how people refer to science as an absolute) and how to manage it
How people in health care professions can mitigate the effects of polarization within their spheres of influence when talking with patients
The event will be moderated by former congressman and current Sid Richardson Foundation President Pete Geren, who will be joined by panelists Bob Lanier, MD; Erin Carlson, DrPH, MPH; Tracey Rockett, PhD; and TCMS Secretary-Treasurer Triwanna Fisher-Wickoff, MD. The keynote speaker will be public affairs consultant and presidential historian Kasey S. Pipes, and the event will also feature Dr. Pickell and UNT System Chancellor Michael Williams, DO, MD, MBA.
The Tarrant County Medical Society is a professional organization that has been dedicated to the improvement of the art and science of medicine for the residents of Tarrant County since 1903. TCMS serves over 4,000 physicians, residents, medical students, and Alliance members, and is a component society of the Texas Medical Association.
Tarrant County Academy of Medicine was incorporated as a 501(c) (3) organization in 1953 to work in conjunction with the Tarrant County Medical Society. TCAM was created to enhance medical education, support community wellness, and preserve Tarrant County’s rich medical history.
“‘Angela’ was stuck. Osteoarthritis in her left hip was holding her hostage.”
Join us as we pick up on Project Access patient Angela’s story in Angela – Part II. You can readAngela – Part I here to learn how Project Access partnered with NTACHC to connect her to a medical home and access to critical presurgical clearance.
After years of debilitating osteoarthritis in Angela’s hip, after overcoming the roadblocks of stress tests and lack of basic medical care through Heart Center of North Texas and NTACHC, it was time for the pain to go away. Project Access volunteer Dr. Mark Woolf of Arlington Orthopedic Associates agreed to perform the hip replacement, believing it was absolutely necessary to Angela’s recovery.
Project Access coordinated the surgery at Baylor Orthopedic and Spine Hospital at Arlington, where U.S. Anesthesia Partners – Arlington Division would provide anesthesia. It was on the docket.
No matter how anticipated a surgery may be, though, there is always a level of anxiety that rises as it draws closer. We wonder if it will help our pain, if our doctor cares about us as individuals. We wonder if this is truly the answer we’ve been searching for.
As soon as the surgery was complete, any fears Angela carried with her were wiped away. She remembers the process being seamless and was overwhelmed by Dr. Woolf’s attentiveness.
“He visited me often; he came on my last day at the hospital to check on me and ask how I was doing,” Angela says. “He had already volunteered so much of his time for the surgery, and he continued doing so!”
After she healed from the hip replacement, everything changed. Angela now has a new job and is able to go to family gatherings and care for her house – things that arthritis had once taken from her. She says she is motivated by the prospect of a future that is not dominated by pain and that everyone who helped her get the surgery is like “God’s healing hands on earth.”
“Being able to have had this surgery has been a blessing for me and my family and is the most wonderful gift anyone could have received,” Angela says. “I will always be thankful for Project Access because they guided me through this whole process and helped so much.”
How can you access specialty care when your most basic medical needs are going unmet?
“Angela” was stuck. Osteoarthritis in her left hip was holding her hostage. The 52-year-old mother of three had to stop attending family gathering and doing performance-based tasks because the pain was too extreme.
“I felt overwhelmed and frustrated because I would wake up with intentions of getting things done but then as I started moving the pain in my hip was so severe that I had to completely stop what I was doing,” she says. “I could not even sit comfortably without having pain.”
The burden was even greater than that, though – she was no longer able to help her husband of 26 years support the family. Working was impossible when even household chores caused too much pain.
She sought treatment with rheumatologists as self-pay when she could afford it, but there was only so much they could do. She needed surgery.
Angela was frustrated; she felt like she was stuck in a never-ending cycle. Her family was suffering both financially and emotionally because of her hip problem, yet she could not rectify the situation because the cost of medical care was just too high.
And though Angela did need the hip replacement, her arthritis was only one piece of her medical puzzle. While she had been able to access some rheumatology care, she did not have a primary care physician to manage her routine care, or the comorbidities associated with her arthritis.
Project Access had a bigger part to play than solely connecting her to a volunteer. Angela needed more services, and we were determined to find them for her.
Since Angela did not have a primary care physician, it was important establish her with one so they could address her numerous secondary issues. NTACHC seemed to be a good fit, and Project Access was able to connect her to their care. NTACHC provided routine checkups and preoperative testing, and Project Access worked with them to guide Angela through the hoops of surgical clearance.
Finally, it was time for the pain to go away.
Tune in tomorrow to hear the rest of this patient’s story in Angela – Part II.
This piece was originally published in the January/February 2022 issue of the Tarrant County Physician. You can read find the full magazine here.
Our nation is beset by radical polarization and erosion of trust. On Saturday, February 19th from 8:30 to 1:00 p.m., Tarrant County Medical Society’s Ethics Consortium will present a CME symposium entitled “Healthcare in a Civil Society 2022” that will explore the factors that have contributed to our present state of bifurcation.
While political discourse has always been polarized, our ability to voice divergent points of view and find common ground has been a hallmark of American democracy, and an important reason why it has worked.
Healthcare policy has been one topic on which we have been able to find common ground. Starting in World War II, trade unions sought alternatives when Congress passed the Stabilization Act (1942), which prohibited employers from increasing wages to their employees. Successful lobbing led Congress to include a provision making health insurance tax deductible to employers, but not to individuals.1 In 1965, Congress established the Medicare and Medicaid programs, thereby creating basic health insurance for the elderly and poor. In both cases there was broad bipartisan support. When Congress passed the Affordable Care Act in 2010, however, not a single Republican voted for it. What happened in those 45 years that transformed healthcare policy from something broadly bipartisan to incredibly divisive?
One reason Medicare and Medicaid achieved bipartisan support is that in 1965, Congress looked and behaved differently. John Dingell, a 60-year congressman from Michigan, noted that when he began serving in the House in 1955, members saw themselves first as representatives of their state, second as representatives of an institution (the House or the Senate), and only third as members of either party. By the time he left Congress in 2015, the order had reversed.2 Furthermore, in the 1960s, we still had left-leaning Republicans and right-leaning Democrats. Crossing party lines was common. People with opposing viewpoints knew each other because they met together, ate together, and socialized together. The result was good legislation achieved by compromise and trust. This is no longer true. While some congressional leaders continue to work well with people “across the aisle,” this has become more the exception than the norm.
If the political process has created a breeding ground for polarization, the advent of “news on demand” has catalyzed it. People can get the “news” they want when they want it from the sources that provide what they want to hear. There is no incentive for these sources to present complex issues in a balanced or nuanced way. Why should they?
By 2014, Pew Research noted that 92 percent of Republicans were to the right of the median Democrat, and 94 percent of Democrats were to the left of the median Republican.3 It’s certainly worse now. While appealing to their bases, each side fails to take into consideration the fact that, in science, what we believe to be true today may be wrong tomorrow. Political leaders have conveyed or distorted information and created policy based on an incomplete understanding of the facts to the detriment of public health. And the medical community hasn’t always been helpful. Our failure to distinguish accurately and consistently between what we know, what we think we know, and what remains a mystery about the current virus, has undermined our messaging to a politically charged and skeptical public.
The public’s reaction to the COVID-19 vaccine serves as a classic example. Many people allowed their position regarding the vaccine to be informed by political narrative rather than by scientific evidence. Lost in the rhetoric is the amazing story of Hungarian-born biochemist Katalin Karikó who, while working as a researcher at the University of Pennsylvania over 25 years ago, had a vision that mRNA could be leveraged for therapeutic effect. Over the last 15 years she nurtured that vision and refined the technology until it became a cure in search of a disease. With COVID-19 it had its disease. How do you put that in a sound bite? And if you manage to, how does it make it past the political noise?
It would be disingenuous to blame this polarization on any single event like the Affordable Care Act or the COVID-19 pandemic. They didn’t cause it. Metaphorically speaking, they are the hurricane that washes ashore and, in its aftermath, reveals off the coast a long-lost pirate ship. The pirate ship was always there, under the surface, but now everyone can see it.
But there is hope. Patients continue to trust us – the physicians they know – even if they are wary of our media representatives. In fact, because physicians adhere to an ethical code dating back over two millennia, we continue to be among the most trusted professionals in modern society, often jockeying with nurses for the #1 position.4 We have a fiduciary responsibility to our patients, and they know it. Our ethical obligation is to serve them – not an insurance company or a hospital, and certainly not a political party.
I call attention to this issue because it will be the focus of Healthcare in a Civil Society 2022. This CME event will explore how we got to this point and begin to chart a path forward. Kasey Pipes, a public affairs consultant, presidential historian, and former speechwriter for George W. Bush, will help us identify the factors that have contributed to polarization. Pete Geren, former congressman and current president of the Sid Richardson Foundation, will again moderate the expert panel that will address:
How the media influences public opinion and promotes polarization and mistrust
The impact of polarization on the public trust and public health
How polarization creates conflict (e.g., in how people refer to science as an absolute) and how to manage it
How people in health care professions can mitigate the effects of polarization within their spheres of influence when talking with patients
The event includes a breakout session allowing participants to explore the topic more deeply in small groups.
One thing I enjoy about being a physician is interacting with a diverse group of people. Part of the challenge for me is understanding where my patients are coming from and meeting them where they are to help them achieve their health goals. I make a concerted effort not to see my patients as “cases” – as diseases to be treated – but as people to be valued and loved. I think this ethos underlies our vocation, and it’s one of the reasons why medical professionals continue to enjoy the public’s trust. And it’s this trust that will help us neutralize the polarizing influences our political rhetoric has on public health. Join us in February and help us explore this important topic more completely.
About Healthcare in a Civil Society
Healthcare in a Civil Society is an annual forum sponsored by the Tarrant County Medical Society’s Ethics Consortium. It seeks to engage leaders of varying perspectives in a civil conversation focusing on the healthcare issues that are important to our community devoid of the rhetoric that often undermines these conversations.
References
1. Feldstein, Martin and James Poterba, editors. Empirical Foundations of Household Taxation. National Bureau of Economic Research. University of Chicago Press, 1996. p. 137. ISBN: 0-226-24097-5. http://www.nber.org/books/feld96-1. Conference Date: January 20-21, 1996.
2. Seib, Gerald. “Gerrymandering Puts Partisanship in Overdrive; Can California Slow It?” Wall Street Journal. November 29, 2021. Seib paraphrased Dingell’s comments in the article.
3. Pew Research Center. “Political Polarization in the American Public: How Increasing Ideological Uniformity and Partisan Antipathy Affect Politics, Compromise and Everyday Life.” June 2014.
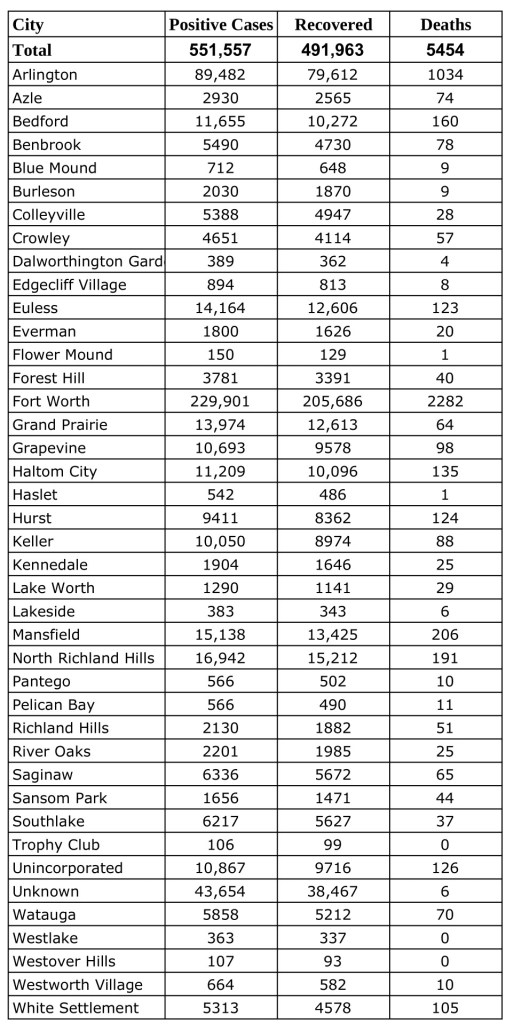
Data from Tarrant County Public Heath’s (TCPH) report of COVID-19 activity in Tarrant County updated Tuesday, February 15, 2o22.Find more COVID-19 information from TCPH here.
*These data are provisional and are subject to change at any time.
Deaths and recovered cases are included in total COVID-19 positive cases.