This article was originally published in the May/June issue of the Tarrant County Physician. You can read find the full magazine here.
My stomach somersaulted as I sipped on another cup of coffee, preparing for a long night of studying cardiology. I realized it was my fifth cup by that point in the afternoon, but I—or more specifically, my grades—could not afford rest. This was my first semester of medical school, when I struggled to see if I truly belonged. It seemed as if everyone around me was adjusting so well, making friends and staying on top of the material, while I was getting buried underneath hundreds upon hundreds of PowerPoint slides each week and felt like I was losing touch with what the art of Medicine meant to me. Whenever this feeling stirs up, I reflect on the experiences that remind me of the humanity behind Medicine.
“Can you help me?” asked one of the residents on the shift. I was part of that summer’s Project Healthcare team, a group of pre-health students volunteering at the emergency department of Bellevue, the country’s oldest hospital. As a volunteer who constantly felt self-conscious about being in the way, I was eager to help. I held an emesis container as the patient, a woman in her 30s, vomited. Afterward, I conversed with her and discovered she was in the ED due to severe abdominal pain. “Maybe it was the spicy food I ate,” she speculated. The resident returned to the bed, preparing to insert a nasogastric tube. As he explained the procedure, the patient became nervous, fearing the pain that was about to compound what she already felt. She asked me if I would hold her hand during this procedure, which I agreed to do. Although I could not alleviate her medical issue, I felt honored and humbled. The patient placed trust in my presence and allowed me, for a brief moment, to provide comfort through physical touch during a painful procedure.
During my undergraduate years, I also volunteered at MD Anderson Cancer Center. I had the opportunity to assume different roles, but the one that shaped me most was being an in-patient unit volunteer. This entailed visiting patients on the floor I was assigned to and seeing if they were in the mood to converse. As someone who primarily spent time with my peers, I pushed myself out of my comfort zone and learned how to strike up conversations with individuals of different ages from varying walks of life. While I felt a slight wave of nervousness every time I knocked on a door, I became more confident in my ability to interact with patients. Although time to converse with patients is much more limited now that I am a medical student instead of a volunteer, I hope to carry over the conversational skills I developed to establish rapport and instill trust in my future patients.
These experiences shaped my time before medical school. However, as a pre-clinical medical student, it is still important for me to seek experiences that show me what type of physician I would like to be. An activity that I have found incredibly rewarding is writing letters advocating for the release of individuals at immigration detention centers for medical reasons during the COVID-19 pandemic. I review relevant patient medical records and compose the letter in collaboration with an attending physician and an attorney. Not only do I learn more about the medical conditions of the patients but also how I can apply the knowledge I am spending years gaining to help improve someone’s environmental conditions.
The science behind Medicine has allowed us to achieve great feats in the prevention and treatment of disease, such as the creation of hemodialysis and the discovery of penicillin. Thorough knowledge of anatomy, physiology, and pathology is foundational in Medicine but is insufficient in our role as physicians. We see people in their most vulnerable states and owe it to our patients—and ourselves—to seek experiences that show us what it means to be human beyond the biology of our bodies.
This article was originally published in the May/June issue of the Tarrant County Physician. You can read find the full magazine here.
by Shanna Combs, MD, TCMS Publications Committee
I did not get into medical school.
I failed my oral board exams.
I lost my job.
It all sounds like the trailer to an incredibly sad movie. But the reality of the situation is I am a board-certified obstetrician gynecologist who has the best job ever. So how did I get here?
“Everything will be okay in the end. If it’s not okay, it’s not the end.”
These are the words I discovered many years ago when a friend was going through a hard time, and it is still a phrase we shoot back and forth when times are tough and not going the way we planned. This is the same friend that picked me up after receiving my rejection letter the first time I applied to medical school. I was not allowed to wallow at home alone—a night of dancing was in order.
Once the dust settled on the acute shock of “not getting in,” I had to decide if this is truly what I wanted to do. I had been a ballet dancer for almost my whole life and was making my income as a dancer, teacher, and rehearsal coach, as well as working at the community college in the physics lab. Such is the lifestyle of an artist and their multitude of jobs.
Upon not getting into medical school, I initially thought about working in education with the goal of teaching ballet. Ultimately though, the call to Medicine was too strong, so I re-took my MCAT, took a biochemistry course, and set my path toward reapplication the next year. I cast a broader net and, in the end, I obtained the privilege of placing “MD” after my name.
Fast forward a few years. I completed my residency in obstetrics and gynecology, passed my written board exam, and began my career as an attending physician. I found my way back into teaching as an assistant professor for medical students and residents. (Guess that career in education was always going to be there.) During this time, I collected my cases and prepared for the next step in board certification—the oral board exam.
Since you read the opening lines, you already know the outcome. Let’s just say, I knew I had failed the minute I walked out of the exam. “Everyone says that” is what I kept being told, but the following week I discovered the truth. It was a difficult time for me. I went through some frustration before I got to acceptance, and there were definitely times where I was not the best person I could be. In the end, I dusted myself off again, pulled up my big girl pants, and began the process for taking the exam again the next year. After multiple reviews of my case list, many practice exams/pimping/torture sessions, I walked in for my second try at the oral board exam.
I left the exam with a vastly different feeling. I knew I had passed. The following week, while driving back from Colorado with my parents, I got the good news that FACOG could also go behind my name. My mom made me pull over, and somewhere on the side of the road in rural New Mexico we got out of the car to dance and celebrate my success.
Fast forward a few more years, and we were hit with the global pandemic: COVID-19. The world as we knew it was changed forever. Little did I know that my personal world was soon to change as well. A few months into the pandemic, I was notified that the clinic I worked for had terminated my contract without cause. I lost my job. How does a busy obstetrician gynecologist lose their job in the midst of a global health crisis? I will never know—that is the problem with the phrase, “without cause.”
In life there will be successes and there will be failures. We always talk about the successes but almost never talk about the failures.
Once again, I found myself wondering what the next phase in my life would entail. I remembered not getting into medical school and wondering if I even wanted to be a doctor anymore. I had worked so hard to get to where I was, yet I was questioning it all over again. Soon after finding out I had lost my job, a friend told me, “You know, you really have not been happy for the past year or two. Maybe this is just what you needed.” Harsh words to hear at first, but in the end, she was right. So, once again I dusted myself off, put on my extra big girl pants, and looked for what I was going to do next.
I have found true joy in working in the field of women’s health, but I always had a special interest in taking care of kids and adolescents. Too often this population gets lost in the shuffle. I am now happy to say I have found a new landing spot in pediatric and adolescent gynecology. Young ladies go through many changes during their young lives and even more so during the transition of puberty. I frequently say, “Puberty is hard,” and I am now able to provide the care and support these young ladies need.
In life there will be successes and there will be failures. We always talk about the successes but almost never talk about the failures. However, it is within these moments that you learn the most. So, why not talk about your failures? I have truly found the honesty of my inner self when I fail. I never thought I would be where I am today a year ago, five years ago, or 17 years ago. Yet, I kept rolling with the punches and taking the next step forward always remembering,
“Everything will be okay in the end. If it’s not okay, it’s not the end.”
This article was originally published in the May/June issue of the Tarrant County Physician. You can read find the full magazine here.
I once wrote about my hopes for life after medical school. I would imagine my office decor, my conversations with patients, the time I would spend coordinating their care. The thoughts were all happy and gave me hope when the dark days of medical school cast a shadow over my upbeat mood, when classes took me down the road of insomnia and gave me a near flat affect from studying more than 12 hours a day during exam time. I guess we all looked like zombies immediately before and after our exams, and some even had the fragrance.
Once a girlfriend came to visit me and she stayed at a hotel on the beach. I discovered the pleasure of sitting and enjoying a piña colada and having zero thoughts of gluconeogenesis or small, slow-conducting fibers (protopathic). Denise, the Coyaba hotel, and a piña colada were all little lights for a med student who was over 2,000 miles from home.
There are times during my professional life that I once again feel like I’m over 2,000 miles from home. Denise is now married and living in Ohio. Piña coladas have way too many calories. The Coyaba hotel would require more PTO than I’m able to take. I’m sitting at my dining room table as I write this because stepping back into the office would make me feel like I’m still at work. I started to take an evening walk but turned around when a close friend told me how much my article sucked (the one you’re not going to read). He didn’t actually say that it sucked; he just pointed out how opposite of uplifting or encouraging it was and said, “It’s not your best work.” Thank you, “D,” for your honesty.
Why would I not be the happiest person you could meet? I have a great job. I am happily single and able to go out and meet a girlfriend for coffee any time I want. I see my beautiful daughter on a regular basis (who is working, doing well in school, and enjoying her youth by spending time with her close friends). My mom survived a hospitalization that nearly took her life in 2013 and has never smoked again (I had taken her home on hospice ten days after she was admitted). Heck, I barely have enough bills to qualify as debt. I should be dancing around the whole Grapevine/Colleyville area. But I’m not.
The strange thing about being there for everyone else is that you sometimes forget to keep a little piece of yourself to enjoy—you just give it all away. Yes, this is a “me” problem. I am the one who picks up the phone when I know the person calling is going to vent for the next 30 minutes, but after 20 years of friendship, you make an effort to still “be there” because that’s what friends do. When your very best friend calls and frantically asks for prayer because the vet is coming to put their horse down (which happened two days ago), how do you not take that call? When your mom wants to tell you about a grandkid she’s concerned about and says the stress is overwhelming, are you going to hang up on her? Another friend tells you they are really concerned because they are still having fatigue and shortness of breath since their heart procedure—and this is one of your health-conscious friends. How can you not feel that? Then there is the job that you love doing, but sadly you do it for 12 hours many days. I find myself on long walks, asking, “Am I missing something?” I wonder if there are elderly patients that I could be helping, or if I’m not fulfilling my calling by now being on the “administrative” side of Medicine.
Long walks, good coffee, and two cats have replaced Denise, the Coyaba, and even the piña colada. As I walk along, I play music from the 80s and 90s and look at all of the different trees—I love the long needle pines the best, they look and smell good. I see the cardinals and the other birds flying around and admire how they know the meaning of commitment. On the weekends I spend hours at the coffee shop with the same few people I’ve been meeting there for years (none of us got COVID-19, and almost everyone is getting vaccinated). They give me a special discount at Buon Giorno, just don’t tell anyone. What? They give everyone that same discount for bringing their thermal mug? I look up at the stars and try to find the big dipper, but I live in Grapevine and, you know, light pollution. I run a hot bath and sit there until it’s barely warm. Netflix holds many fond memories from my COVID-19 nights: Shtisel, Sex and the City, The Crown, Girlfriends . . . I really do make the most of each day and try to laugh as much as I can. It’s just been hard to laugh lately, and I wanted to share in case someone else is also having a hard time laughing, or sleeping, or even folding the laundry.
We are the ones who are there for everyone else. Who is there for us? Though my friends and family can drain the very life force from my body, I want you to know that I am here for you. You have sacrificed so much for others, and your colleagues see you. They care even though you thought they didn’t like you. I am struggling a bit these days, as I suspect many of us are after the year we’ve been through.
Perhaps this is just my COVID-19 carb crash, but I am ready for this season to end. I am praying; I like to pray. I am even going to church on occasion . . . not that I care for going to church. But my faith has always seen me through the most difficult of times, and I once again find myself reading Joshua 1:9, knowing that He will be with me wherever I go. I am going to put that and a few other verses on the wall behind my laptop as a reminder that He is always with me. I have friends who do not share my faith, my politics, or my taste in music, but we do share the need to connect, to laugh, and to be heard. Thank you for reading my article and for being one of the lights in a sometimes dark place. Call me any time at 817-798-8087 (text first if you actually want me to pick up). We’re all walking through this—let’s do it together.
This article was originally published in the May/June issue of the Tarrant County Physician. You can read find the full magazine here.
As we start a new year, health care providers should consider a compliance check. Health care laws change, new regulations are promulgated, and advisory opinions1 are issued on a frequent basis. Healthcare policies and procedures need to be reviewed to make sure they are up to date, and organizations may need to undertake certain necessary actions, e.g., updating their HIPAA security policy. Compliance checks are ideally performed at least once a year.
In the past year, for example, the federal Stark anti-referral regulations were amended.2 The Stark amendments made significant changes to the rules, including revising the definitions of “fair market value” and “commercial reasonableness.” In addition, amendments to the HIPAA regulations have been proposed,3 and the Office of the National Coordinator for Health Information Technology (ONC) finalized rules for electronic records that include provisions relating to patients’ access to their medical records.4
For a compliance review, HIPAA issues to consider include, but are not limited to:
Review employee training to confirm it is up to date, including necessary or desirable written documentation;5
Review Notice of Privacy Practices provided to patients – is everything current; do new areas need to be added or sections deleted? Are the explanations of possible uses of patient data correct?
Review the security risk assessment, particularly given the increase in cyberattacks. Review any changes to technology, new equipment such as computers or servers, new software, and what third parties and employees have access to medical records. Has your location changed? Is your security contingency plan still accurate?
Review to verify patient access to their records complies with the new ONC rules and HIPAA;
Determine if there are new business associates to add, business associates that need to be deleted, or agreements amended;
Verify that the named HIPAA privacy and/or security officer is still in that position;
Review the breach reporting policy and make necessary or desirable changes;
Determine if any third-party agreements or business associate agreements have been revised or added, and if so, if the agreements in writing include any amendments;
Assess compliance with state privacy/medical record laws, which often have different provisions than HIPAA.6
In other areas, things to consider include, but are not limited to:
Perform an inventory of third party agreements and verify, for new or amended relationships, as applicable, that an appropriate Stark referral analysis was performed and is up to date and that an anti-kickback analysis also was performed and is up to date, i.e., is remuneration fair market value?7
Update policies and practices to conform to the new Stark rules and any other applicable new or amended federal and state laws;
Review continued compliance with any safe harbors relied on under the Stark rules and/or anti-kickback rules, if applicable, e.g., equipment or real estate leases, personnel service and/or management agreements;8
Confirm employee background checks are up to date;
Confirm federal health care exclusion screening is up to date;
Confirm licensed employees have completed continuing education requirements and any other conditions to maintain licensure;
Inventory leases and any amendments and make sure appropriate documentation is in place, including, if applicable, a fair market value analysis;
Verify record retention policies still comply with current laws and that the procedures are being followed;
Consider whether an audit of the use of appropriate billing codes is necessary;
Verify required licenses are up to date for personnel and any equipment;
Verify compliance with federal and state telehealth laws, if applicable, including any provisions related to COVID-19;
Verify that patient record request policies are up to date and that personnel are complying with the policies;
Verify appropriate due diligence is being performed for applicable laws when new vendors or contractors are engaged.
Your organization should also consult in-house or outside counsel to verify any changes to federal and state laws before beginning the compliance review process. Furthermore, there is value in engaging an attorney and seeking legal advice on the review in order to invoke the attorney-client privilege where possible. The privilege will not protect all documents or all communications, but it provides significant protection during the process for covered communications.9
Again, this “list” is not comprehensive, particularly given the plethora of health care laws that could apply and the complexity of such laws. As an example, this list does not focus on Medicare or Medicaid compliance. Nonetheless, it should provide a reminder for the key areas to cover when conduct a general healthcare compliance check.
References:
1. This article is not intended to be a comprehensive summary of all final or proposed changes to federal and state health laws and regulations. Additionally, given the many types of healthcare providers, the article does not address all possible federal and state laws but is intended to provide an example of the type of questions they should ask.
2. See, e.g., OIG Advisory Opinion No. 20-08 (Dec. 20, 2020) ((regarding a federally qualified health center’s proposal to offer gift cards to incentivize certain pediatric patients to attend rescheduled preventive and early intervention care appointments).
3. 85 Fed. Reg. 77,492 (Dec. 20, 2020).
4. See 85 Fed. Reg. 6,446 (Jan. 21, 2021). The proposed changes largely relate to the new ONC rules regarding access to patient records.
5. See 85 Fed. Reg. 25,642 (May 1, 2020).
6. According to many experts, training should be performed at least annually.
7. For example, the Texas Medical Record Privacy Act has a much broader definition of “covered entity” than HIPAA, being any person who engages in the practice of assembling, collecting, analyzing, using, evaluating, storing, or transmitting protected health information and including any person who obtains or stores protected health information. See also 15 Tex. Admin. Code § 390.2 which lists various statutes that could be applicable to Texas covered entities.
8. The definitions of “fair market value” and “commercial reasonableness” have changed under the new Stark rules that were effective January 19, 2021 (with limited exceptions).
9. The new Stark rules also made changes in these areas.
10. Generally, the elements of attorney client-privilege are: (1) the person asserting the privilege must be a client or someone attempting to establish a relationship as a client; (2) the person with whom the client communicated must be an attorney and acting in the capacity as an attorney at the time of the communication; (3) the communication must be between the attorney and client exclusively; (4) the communication must be for the purpose of securing a legal opinion, legal services, or assistance in some legal proceeding, and not for the purpose of committing a crime or fraud; and (5) the privilege may be claimed or waived by the client only.
This article was originally published in the May/June issue of the Tarrant County Physician. You can read find the full magazine here.
One of my favorite roles as a physician and medical educator is the opportunity to be a mentor. At the TCU and UNTHSC School of Medicine we recently kicked off our 2021 Diversity and Inclusion Mentoring Network Series. As with everything in life, our mentoring network had been put on the back burner due to the COVID-19 pandemic. It was so refreshing to get back into the mentoring groove again with our latest event, even if it was virtual.
Mentoring is a critical piece to the development of aspiring physicians, not just at the medical training level but also at the college, high school, and school age level. Unfortunately, over the past few decades the decision to become a physician has all too often been met with negativity…
. . . too much schooling, too much debt, no time for a family or a life, medical-legal concerns, too much paperwork, financial concerns, and ultimately, physician burnout.
I still remember telling physicians that I wanted to be a doctor when I grew up and immediately hearing how that was not a good career choice, and if they had to do it all over again, they would choose another field. Thankfully, I occasionally met a doctor or two who showed me how much they loved their work and encouraged me in my pursuits. This is why mentorship matters.
During this crazy year of a global pandemic, we have truly seen the importance of our healthcare team members and have even named them heroes. I only hope that this will continue. While our path as physicians is not always easy, I feel that it is an extremely rewarding one, and I want to help others see how amazing it is to be a doctor. Mentorship comes in all forms, and one just needs to be willing to share their guidance and expertise to become a mentor. Mentoring can be formal, peer-to-peer, developmental, instructional, or informal. No matter the form, mentorship is extremely important and provides benefits to the mentor as well as the mentee.
At our recent mentoring event, not only was I able to provide guidance and nurture our up-and-coming physicians, but I was also able to learn a lot about our community. Some of the amazing features of the TCU and UNTHSC School of Medicine Diversity and Inclusion Mentoring Network are that it crosses multiple areas in Medicine, includes mentors from a variety of backgrounds and journeys in life, and is made up of physicians, researchers, administrators, and leaders in the community. In addition, due to the need to meet virtually, it now includes mentors from across the country who have a connection to our school. It was exciting to hear about others’ successes, failures, and varied experiences in Medicine as well as to hear about their “why” for pursuing it as a vocation. It was also refreshing to see the joy on the students’ faces as they were able to interact in small groups with mentors and hear the various pearls of wisdom each one had to share.
By mentoring medical students, you can provide opportunities for growth and professional development, demonstrate the various careers and specialties in Medicine, and give career advice and counseling. Most importantly, though, you can see the enthusiasm for your chosen profession. So, if you need a little more joy in your life, I highly recommend finding a way to be a mentor to those in need of guidance and encouragement. Please feel free to join our Diversity and Inclusion Mentoring Network at the TCU and UNTHSC School of Medicine. As with everything in life, a village can only make you stronger.
When I began searching for internship opportunities needed for completion of my public health degree at UTA, I immediately thought of Project Access Tarrant County.
I originally became aware of PATC when my mom received their services a couple of years ago. Through that experience, I knew that PATC assisted patients with access to specialty medical care, but I was not fully aware of everything PATC did until I started interning. I have always had a passion for helping others and I knew that I wanted my intern experience to be at an organization that truly helped the community and upheld their values. I found just that and more at PATC.
My role is to facilitate and maintain patient re-enrollment; I am able to help patients gather the needed documents to meet our requirements. I also interview new patients via Zoom, completing their enrollment process. I have learned many skills that will be useful in any career I choose after my internship, and I am so glad I have had such a great group of women to help me succeed. I did not expect to have such an important role as an intern but PATC has challenged me in the best way possible.
One of the most rewarding aspects of my internship is following up with patients who have finished their care and hearing about their experiences. There is one patient whose interview I will never forget. This patient was diagnosed with rheumatoid arthritis in her mid-twenties. She had been in severe pain for the past few years, and just recently, PATC was able to help her get a life-changing surgery that will allow her to walk again. During her interview, she shared with me all of the hard times she had endured, times that made her want to give up on life. In that moment, I realized just how big of an impact PATC makes on not just individual patients but their entire families. I was so glad we were able to help this patient, but I also felt amazing knowing I am now part of this organization and can continue serving my community.
“One of the most rewarding aspects of my internship is following up with patients who have finished their care and hearing about their experience.”
Many people are fortunate enough to have access to healthcare, but there are many others who do not have the same opportunity. As a community, it is important that we provide resources to those who are underserved and that we understand their needs. I have been able to experience exactly how PATC is able to do just that not only from an administrative point of view but also from a medical perspective. It takes a village to make it work. From Kathryn, Diana, Angie, and TCMS to the volunteer doctors and their staffs, everyone works together to ensure that they are able to successfully meet our patients’ needs. Hearing patients’ stories about how we have changed their lives and their families is such a heartwarming feeling. There is nothing better than seeing our patients thrive.
by Michael Bernas Scholarly Pursuit and Thesis Program Director
This article was originally published in the March/April issue of the Tarrant County Physician. You can read find the full magazine here.
Have you ever been curious about an unknown in your practice? Do you ever find yourself thinking “what if…”? Have you always been curious about doing a little research, but not sure where to start? If so, you may be interested in participating in a research project with a medical school student from the TCU and UNTHSC School of Medicine.
The program is called the Scholarly Pursuit and Thesis (SPT) course and it is a four-year research project that all students at the school undertake as part of their education. It was designed for students to explore medical research, practice critical inquiry, and use medical information literacy to become patient-centric physicians with life-long curiosity and learning skills. The course begins with students reinvigorating their curiosity and questioning skills. This is followed by some basic research training, including literature searching and appraisal skills, research question development, and human subjects training through the Collaborative Institutional Training Initiative program. Program faculty will help develop these skills and assist students throughout their research projects.
Many students have prior experience with research from their undergraduate or post-college education. During the first year, students work with their mentor to produce a prospectus that is similar to a small research grant application, detailing project parameters. During the next two years students work on projects with their mentors, and in the fourth year they produce a thesis as well as a poster for a public presentation.
Some common questions from potential research mentors include:
What is the role of the mentor? The mentor acts as a guide to the student in the research project. He or she will assist the student in designing the research project and often help with providing data or access to data for research. The mentor will work with the student as they monitor data collection and interpretation, will be available for questions, and will assist the student with the final thesis conclusions.
What areas and topics are appropriate for student research projects?Mentors and projects can come from any field (see Table). The only requirements are that the project is researched effectively, includes some sort of intervention or examination (experiment, chart review, product design, data collection, etc.), has a good plan for analysis of results, and includes a discussion of the results with potential application and questions for the future.
How does a student decide what research project to do? Generally, there are four ways to develop the projects. Firstly, the mentor may already have some ongoing research that the student can join or carve a piece from. Secondly, often mentors have some questions that they have been curious about and want to explore further. Thirdly, students sometimes have their own specific question to start with as the basis for their project. Finally, after some discussion concerning issues and questions in a specific area, the mentor and student can design something completely new. Whatever way the decision is made, communication between the mentor and student helps drive this process.
How much time will this take? Time with the student will vary from project to project and there are no specific program requirements. Overall, the mentor needs to commit to working with the student for four years (projects chosen and designed at approximately end of semester 1 and thesis submitted at approximately end of semester 7). However, during this time, due to obligations and schedules of both, this could mean meeting almost every week in some labs (approximately one hour) to perhaps only meeting every two to three weeks for some clinicians or mentors. As the project progresses, there may be less need for frequent interactions until data review and analysis. We anticipate that mentor-student meetings will also include some “life lesson” discussions and the potential to develop a lasting relationship.
Do I need to have experience as a researcher? No, there are no requirements for prior experience, only your willingness to work with the student.
Does the student need to publish a manuscript on the results? There is no requirement that the students publish a manuscript before they graduate. However, it is the expectation that the majority of student projects will result in publication in addition to abstracts and posters/presentations from project results as appropriate.
What are the benefits to me as a mentor? All mentors will receive an academic appointment with the TCU and UNTHSC School of Medicine. In addition, you get to work with an enthusiastic and curious student for four years, who will perform most of the work. The curriculum design provides education in basic science (year 1) and clinical training (year 2) in an accelerated fashion, producing an experienced mini-physician to enhance your research team. Finally, students will have educational experiences throughout North Texas with the potential to share or expand your research.
How do I learn more? This article is just an introduction. For more detailed information and any questions, please contact Program Director Michael Bernas at m.bernas@tcu.edu.
This article was originally published in the March/April issue of the Tarrant County Physician. You can read find the full magazine here.
The last words I wrote in this journal were printed in January 2020, after a family trip to Disney World:
“I returned to work in this New Year, in this new decade, invigorated. My optimism stems from the smiles of my baby girl and her beautiful mother. It stems from an understanding that our imaginations power our spirit and our spirit powers our hearts. This year, 2020, will be an amazing year for all of us because I will will it to be so. The world is full of magic. We are so blessed to be physicians. I needed a particular princess to remind me of this. Search your feelings, you know it to be true. I hope your year is starting out as well as mine. I pray that all of us can find perspective and optimism somewhere in this world, so that despite the bureaucrats and the obstacles and the hazards along our journey, we can continue to serve our patients in this, the highest of all callings in the Galaxy.”
This was quite obviously written before a viral pandemic spread across the United States, infecting countless numbers of our families, friends, and loved ones, killing over 500,000 Americans. It was written before our world changed forever.
Overwhelmed. Exhausted. Fatigued. These are the emotions that have defined our existence on the front lines of the COVID-19 pandemic over the last year. We have watched helplessly as many of our patients and loved ones have slipped away. We have held the hands of patients who have passed away in respiratory isolation, their closest loved ones on phones and miles away, not allowed into the hospital. But I have seen Joy, when the infection overwhelms but the body and spirit fight on, conquering the virus and returning our patients to health. We have seen families reunited after long battles in the hospital ICU or at home in quarantine. We have seen Hope. We have known Love. I have seen the fantastic power of the human spirit. I have seen God’s love, and the power of prayer. There were moments when I felt that I could no longer fight for myself or anyone else, when the exhaustion would creep into my bones, and leave me battered, bruised, and almost beaten. But we are physicians. And we work with amazing, powerful nurses, medical assistants, medical techs, therapists, and hospital administrators—a formidable health care team. So I saw unexpected acts of bravery, acts of selflessness, moments that were etched into my soul forever. I saw us fight an unknown adversary. I have been privy to courage and honor, as we wrapped our patients in an armor of hope. I have seen hands that are raw from washing and sanitizing and wringing but showed no signs of relenting or retreat or defeat.
And in early January of 2021, at the hospital where I have seen and experienced all of this, there was a moment where my hope was recovered, where I became recharged and ready to step back onto the battleground. I saw the proverbial light at the end of the tunnel, the sun peeking over the horizon at the end of a cold dark night. The promise of a new day. The vaccine.
“Overwhelmed. Exhausted. Fatigued. These are the emotions that have defined our existence on the front lines of the COVID-19 pandemic over the last year.”
As I received that second dose, I wondered how any of us survived this year. I wept tears of joy, thinking that I finally knew in that moment that we would make it through this war. The tears burned with the memory of all those we have lost. It didn’t need to get this bad. Why did we have to lose so many? And how many more will we lose? The answer depends now on our resolve. We must resolve to vaccinate as many of our patients as we can as soon as possible. As a medical community, we should assist our public health departments, hospitals, clinics, and our federal, state, and local governments to roll out these vaccines with great efficiency. The only way we will win this war now is by vaccinating the masses and following the public health guidelines to wash our hands, distance, and wear masks.
I returned to work in this New Year, 2021, reinvigorated. My optimism stems from the smiles of my colleagues, which have been renewed with hope that the tide is turning. My optimism stems from an understanding that our imaginations power our spirit and our spirit powers our hearts, and that science and ingenuity and heart will prevail with the advent of this vaccine. This year, 2021, will be an amazing year for all of us because I will will it to be so. The world is full of magic. We are so blessed to be physicians. Search your feelings, you know it to be true. I hope your year is starting out as well as mine. I pray that all of us can find perspective and optimism somewhere in this world, so that despite the ill effects of COVID-19 on all of our lives, and the obstacles and the hazards along our journey that was 2020, we can continue to serve our patients in this, the highest of all callings. I want to thank all of my colleagues and compatriots who have shared this year with me and my family. We have shown that together we are stronger, and we will overcome. My name is Hujefa Vora, and this is the Last Word.
This article was originally published in the March/April issue of the Tarrant County Physician. You can read find the full magazine here.
Medical school has one primary goal: passing on humanity’s medical knowledge to a new generation. There are a few challenges to accomplishing this goal. First is a static problem, i.e., the sheer magnitude of information. Second is a dynamic problem, i.e., the rate of change of this information. Humankind’s medical knowledge is growing and being refined at an incredible rate. These forces are constantly at play in medical school, and they only become more obvious the deeper one’s understanding of a topic becomes. Learning more means absorbing all of the idiosyncrasies and all of the exceptions as well as confronting the burden of complexity. This is a problem that our species has been dealing with forever. Just take the ancient story of Adam and Eve; life was simple until they ate the apple and had to deal with the consequences of knowledge.
“Drinking from a fire hydrant” is the analogy often used to describe the intensity of learning in medical school. This is what medical students volunteer for beginning in year one, and it will continue until we retire. The best and only solution is old-fashioned hard work and careful thinking. This is the reality that you have to accept if you choose to be a doctor. Unfortunately, this same reality of drinking from a fire hydrant now applies to our whole society that is woefully unprepared for the flood of medical knowledge and information.
Our society’s fire hydrant does not come in the form of a pathology textbook, but in the form of the Internet and social media. Everyone is bombarded with health content, and the mishandling or misinterpretation of this information has many potential problems. These can range from wasted patient resources to creating false expectations—they can even lead to physical harm. As doctors we become familiar with information overload and have the opportunity to develop strategies to handle it. We learn to be skeptical, research thoroughly, test our assumptions, and rely on experts. It is sometimes easy to assume the whole world has some of these strategies too, but this is obviously not the case. I don’t even need to give a specific example, just browse Twitter or Facebook for a few minutes and I am certain one will present itself. Ideally, everyone would have instant access to a healthcare worker to help them navigate the things they see online. This is currently impossible, so many patients will have to sort through the overload of truth and misinformation on their own. In light of this problem, I am reminded of a famous quote by a pillar of our profession:
“One of the first duties of the physician is to educate the masses”1
–Sir William Osler.
I believe that we can benefit society by educating our patients about strategies to sort through medical information they find online. Strategies like having some skepticism toward this information, researching it through reputable sources, and trying to disprove something they see on social media before they believe it. Strategies that we have had the opportunity to develop through our medical education.
I am like most second-year medical students and I am probably too eager to share what I have learned with those around me. What has been surprising to me is that most of the health questions my friends and family ask or the incorrect assertions I hear are different from what I expected. For every time I get to explain how someone’s medication works, there are five times of disputing something someone saw on social media. I understand that not everyone has the benefit of medical school, but I fear that the massive amount of online health information has the potential to cause harm if people do not have basic strategies to handle it.
In closing, I will admit that the quote I used was not complete. The full quote says that “One of the first duties of the physician is to educate the masses not to take medicines.” I completely misrepresented the quote because it demonstrates how the simplest strategies can be used to check the validity of something you read. One Google search is all it takes to gather evidence that I was not being completely truthful with Dr. Osler’s claim. That being said, if Osler were alive today, I believe he would agree with the sentiment that “One of the first duties of the physician is to educate the masses not to believe everything they see online.”
1Osler, William, Robert Bennett Bean, and William B. Bean, Sir William Osler Aphorisms: from His Bedside Teachings and Writings, (New York: Schuman. 1950).
This piece was originally published in the March/April issue of the Tarrant County Physician. You can read find the full magazine here.
We can all learn in many ways from the intellect of Greece and Rome. This principle applies to infectious events which took place in those societies in the long distant past and were well documented by ancient writers in their descriptions of early epidemics.
In these difficult COVID-19 times we still rely on these empiric approaches obtained from past management of epidemics in times of war and peace. We have also learned how to complement this management with careful scientific research and study to develop more specific treatments and successful vaccination programs. Additionally, we have learned that it is important to have consistent, well-coordinated public education.
The Athenian Plague
This plague occurred in the setting of the Peloponnesian War, a long war caused by conflicts between the states of Athens and Sparta and their allies.1,2,3 Democracy originated in Athens in 500 B.C. It was brought about through the assembly of the 500, a group chosen to make important decisions regarding essential affairs of the city.
Athens, expanding into Attica and controlling the surrounding Ionian Islands, established the Athenian (also called Delian) League and built a naval empire. It became wealthy by exporting olive oil and wine and trading silver from nearby mines. It thrived under Pericles, a leader who built the Parthenon and encouraged culture and creativity in the city.
Sparta, by contrast, was a land-locked military state comprised of rigorously trained soldiers. It was ruled by kings that controlled underclass servants. They also expanded into neighboring city-states. Athens and Sparta became rivals that clashed due to their different styles of government and policy.1,2,3
The Spartans also built their own defensive alliance, the Peloponnesian League, which antagonized the Athenian League.
Athens protected its neighboring states from Spartan attacks and built walls between Athens and Piraeus (also spelled Peiraieus). To prevent further clashes Athens and Sparta signed a peace agreement, but the Spartans and their allies disliked the democratic and expansive Athenian approach and felt it needed to exercise greater restraint. Therefore, in 431 B.C., Spartan troops and allies made several incursions through Attica into Athens. This started a long series of battles with inconclusive results that were fought for 26 years in different sites either by land or sea. This ruined the Greek economy, adversely affected the lives of many families, and changed the course of Greek history.
This so-called Peloponnesian War has been described at length by the brilliant general and historian Thucydides and is still studied by contemporary researchers.1,2,3 The final downfall and cultural deterioration of Athens was caused by the combination of damage to its fleet after a failed invasion of Sicily and by the enormous loss of life caused by the Athenian plague.
This epidemic started in the second year of the Peloponnesian War, after the Spartan invasion and siege of Athens in 430 B.C. As reported by Thucydides, this disease appeared suddenly, with high fever, red eyes, sore throat and tongue, hoarseness and cough, vomiting bile, severe diarrhea, restlessness, purplish cutaneous pustules and ulcers, and also lesions over fingers and toes, sometimes with gangrene. Recent review articles suggest that the most likely epidemiological diagnosis was smallpox, with typhus being less probable.5 It did not appear to be bubonic plague.
Thucydides described the overcrowding in the walled city of Athens where he proposed the important concept of contagion of disease. He defined it as the transmission of illness from a sick person to a healthy individual. He was then influenced by the ideas of Hippocrates, who claimed that the secretions of a sick individual would contaminate the air during an epidemic.6
This proposal anteceded by thousands of years Pasteur’s and Koch’s observations on germ transmission. Thucydides also noted that death could occur on the seventh or eighth day of disease but observed that those who recovered might acquire partial immunity and did not die from a second round of disease.
Waves of infection affecting the local population led to the death of one-third of Athens’ inhabitants. So many of the dead remained unburied that at times the corpses piled up on the street. Thucydides blamed this on lack of humanitarian response of the survivors. He himself, who got the disease and recovered, suggested avoiding overcrowding and exposure to the sick; however, Pericles, who was leading Athens at the time of the infection, suggested the transfer of rural refugees to the walled city. This increased the risk of their contagion. He also became a victim of the illness, from which he did not survive.
Euripides, who also lived at the time of the war in 415 B.C., described in an allegorical drama, “The Trojan Women,” a prophecy for a tragedy that predicted the disaster that would befall Athens after the failed Sicilian campaign when Athens lost her entire fleet, and a large number of young sailors became enslaved. This was a message on bad war planning in a Greek drama written in the fifth century B.C.7
As Rome conquered Greek territories, the Roman Empire in turn was deeply influenced by Greek culture, which became integrated into buildings and sculptures. The Roman Empire was also influenced by their religious beliefs and images. Hellenistic centers created in Alexandria and in cities of Asia Minor were later absorbed and integrated into Rome.
Antonine Plague
The first recorded epidemic in Roman times was called the “Antonine plague.” It appeared in A.D. 165 to 180, and waves of disease followed between 211 and 266. To Galen, the observant Greek physician, the victims presented with fever, chills, sore throat, bloody diarrhea turning black, and a pustular rash on the ninth day consistent with smallpox. The acute phase of the disease lasted two weeks. It affected large numbers of Roman residents, with high mortality due to the density of population and excess of waste and sewage.4 It killed Marcus Aurelius Antoninus and Lucius Verus, the two reigning emperors.8 It is believed that the Roman soldiers brought the organism from Egypt and the Middle East into Rome.
In those times, early Christians were persecuted for refusing to honor the Roman gods. However, they endeared themselves to the sick for providing them with some form of care.
The Roman Empire later became stretched financially by excessive warfare, rapid emperor turnover, and increased civil wars. Rome was eventually sacked by invading Visigoths in 410, and the last western emperor was deposed in 476 A.D.
Justinian Plague
The Eastern branch of the Roman Empire was then established with Constantinople as the capital of what was to become the Byzantine Empire. A different type of plague appeared in 541 A.D. during the Emperor Justinian’s rule in Constantinople. Justinian (527- 565 A.D.) is known for military campaigns, civil law reforms (he wrote Codex Justinianeus), and for creating important buildings (Hagia Sophia in 562 A.D.).
It has been claimed that this plague caused the loss of up to one-third of the total Mediterranean population. It may have presented in recurrent intermittent waves that, lasted up to 200 years. It has also been suggested that it led to the waning of the Roman Empire and the advent of the Middle Ages.11
The historian Procopius (500 – 565 A.D.) described the appearance of this plague in Pelusium, Egypt, on the Eastern Nile, and its spread to Alexandria and later to Constantinople, Asia Minor, and the Middle East.
Procopius observed subjects with fever. They had “large painful swellings” in groins, armpits, and neck followed by delirium, black blisters, and vomiting, which frequently led to death. Occasionally, he noted, “The lumps start draining pus, the fever subsides, and the person sometimes may even recover.” There were similar reports from other observers at that time, like John of Ephesus.8
We know now that rats carrying fleas were brought in by ships supplying grain from Africa to Constantinople. Bubonic plague’s causative organism, Yersinia pestis, has been isolated and its DNA sequenced.10 This was obtained from tombs in sixth century Bavaria. It was found to represent a distinct genetic lineage originating from a different rodent reservoir for this pandemic than the one occurring in medieval Europe.
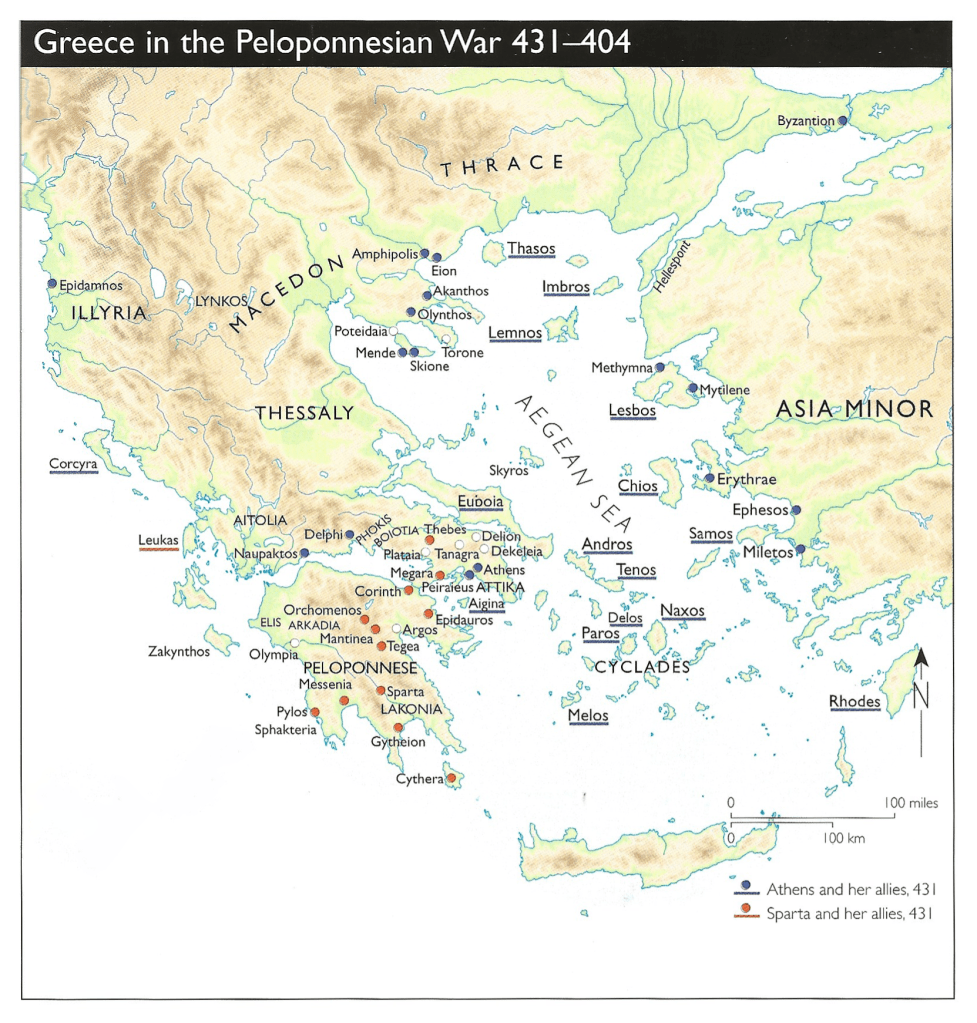
States controlled by Athens (blue) and Sparta (red) at war1
A recent detailed research paper by a multidisciplinary group questions the Justinian plague as being such a watershed event in history.9 After examining a series of independent fields of study such as papyri, inscriptions, and coins as well as pollen and burial sites, the authors conclude there is little evidence that the Justinian plague was a major driver of demographic change in the sixth century Mediterranean area. These findings indicate this plague was therefore very different from the devastating second pandemic that presented later in the Middle Ages.
We have learned that two ancient pandemics, the Athenian plague in early Greece and the Antonine plague in early Rome, appeared in cities with overcrowded populations. Their disease presentation at the time indicated exposure to a highly infectious, rapidly spreading agent that caused an acute, devastating disease of high mortality. Both epidemics had similar clinical presentation, in which fever and mucosal and pustular skin lesions predominated. We know now that they most likely represented smallpox, and this disease became airborne from mucosal lesions but could also spread by contact of skin ulcerations. It affected people of all social classes, including leaders and emperors. Such a contagious disease would have made patient care very risky and difficult. No wonder the corpses piled up on the streets of Athens!
Smallpox ravaged the entire world. It reached the Americas, including the U.S. and Mexico during colonial times. It decimated the Aztecs when the Spanish conquistadors arrived in Tenochtitlan, as the Aztecs had no previous exposure to this virus.
After Jenner published his spectacular results with vaccination in 1798, smallpox immunization was eventually adopted all over the world and the disease was completely eradicated by 1980.
Prevention of social gatherings was applied during the severe 1918 flu pandemic with measures such as closures of schools, shops, and restaurants, mandated social distancing, and home quarantining when needed. In cities in which these multiple recommendations were implemented earlier and kept in place, transmission of disease and mortality were reduced. This beneficial result demonstrates that avoidance of contact between individuals can be helpful in controlling transmission of highly contagious disease, which is why this approach is being used for the management of the COVID-19 virus.
References
1RMorkot-HistAtlas Ancient Greece- Penguin 1stEd 1996
2D Kagan – The Peloponnesian War – Viking 2003
3VHanson-A War Like No Other- RandomHouse2006
4ErinyHanna-Cities,Disease,Trade, Epidemics in Roman Empire Vanderbilt-Uni 2015
5RLittman-The plague of Athens. Epidemiol and Paleopathology. Mt.SinaiJMed 76:456
6HippocraticWritings:The natureof man Penguinclassic1983
7Euripides TheTrojan women Signet classic 1998
8GKohn; Encyclopedia of Plague and PestilenceWordsworth1995
9LMordechai-The Justinian Plague An Inconsequential Pandemic? PNAS 116-5125546
10D Wagner – Yersinia Pestis and the Plague – Genomic Analysis Lancet 14 April 2014
11Bassareo – Learning from the past in Covid-19 Era – Post Grad Med J 114:633
Images
1Souza, Philip De, The Peloponnesian War, 431-404 BC., (Oxford: Osprey, 2002).